

Costs and Benefits Associated With Transradial Versus Transfemoral Percutaneous Coronary Intervention in China
- PMID: 27107136
- PMCID: PMC4843527
- DOI: 10.1161/JAHA.115.002684
Costs and Benefits Associated With Transradial Versus Transfemoral Percutaneous Coronary Intervention in China
Abstract
Background: Transradial percutaneous coronary intervention (PCI) has been increasingly adopted in clinical practice, given its potential advantages over transfemoral intervention; however, the impact of different access strategies on costs and clinical outcomes remains poorly defined, especially in the developing world.
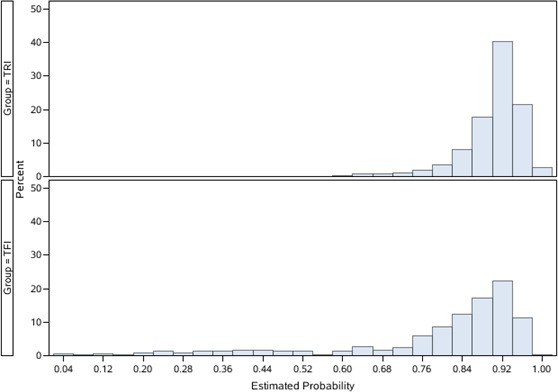
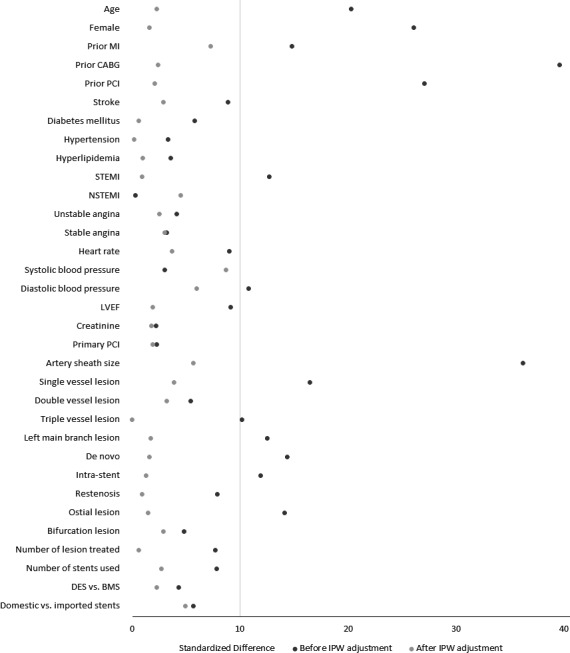
Methods and results: Using data from a consecutive cohort of 5306 patients undergoing PCI in China in 2010, we compared total hospital costs and in-hospital outcomes for transradial intervention (TRI) and transfemoral intervention. Patients receiving TRI (n=4696, 88.5%) were slightly younger (mean age 57.4 versus 59.5 years), less often women (21.6% versus 33.1%), more likely to undergo PCI for single-vessel disease, and less likely to undergo PCI for triple-vessel or left main diseases. The unadjusted total hospital costs were 57 900 Chinese yuan (¥57 900; equivalent to 9190 US dollars [$9190]) for TRI and ¥67 418 ($10,701) for transfemoral intervention. After adjusting for all observed patient and procedural characteristics using the propensity score inverse probability weighting method, TRI was associated with a lower total cost (adjusted difference ¥8081 [$1283]). More than 80% of the cost difference was related to lower PCI-related costs (adjusted difference -¥5162 [-$819]), which were likely driven by exclusive use of vascular closure devices in transfemoral intervention, and lower hospitalization costs (-¥1399 [-$222]). Patients receiving TRI had shorter length of stay and were less likely to experience major adverse cardiac events or post-PCI bleeding. These differences were consistent among clinically relevant subgroups with acute myocardial infarction, acute coronary syndrome, and stable angina.
Conclusions: Among patients undergoing PCI, TRI was associated with lower cost and favorable clinical outcomes compared with transfemoral intervention.
Keywords: coronary artery disease; cost; health services research; interventional cardiology; outcomes research; percutaneous coronary intervention.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Brueck M, Bandorski D, Kramer W, Wieczorek M, Höltgen R, Tillmanns H. A, randomized comparison of transradial versus transfemoral approach for coronary angiography and angioplasty. JACC Cardiovasc Interv. 2009;2:1047–1054. - PubMed
-
- Pristipino C, Trani C, Nazzaro MS, Berni A, Patti G, Patrizi R, Pironi B, Mazzarotto P, Gioffrè G, Biondi‐Zoccai GGL, Richichi G. Major improvement of percutaneous cardiovascular procedure outcomes with radial artery catheterisation: results from the PREVAIL study. Heart. 2009;95:476–482. - PubMed
-
- Yang Y‐J, Kandzari DE, Gao Z, Xu B, Chen J‐L, Qiao S‐B, Li J‐J, Qin X‐W, Yao M, Wu Y‐J, Yuan J‐Q, Chen J, Liu H‐B, Dai J, Chen T, Wang Y, Li W, Gao R‐L. Transradial versus transfemoral method of percutaneous coronary revascularization for unprotected left main coronary artery disease: comparison of procedural and late‐term outcomes. JACC Cardiovasc Interv. 2010;3:1035–1042. - PubMed
-
- Jolly SS, Yusuf S, Cairns J, Niemelä K, Xavier D, Widimsky P, Budaj A, Niemelä M, Valentin V, Lewis BS, Avezum A, Steg PG, Rao SV, Gao P, Afzal R, Joyner CD, Chrolavicius S, Mehta SR. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet. 2011;377:1409–1420. - PubMed
-
- Hamon M, Rasmussen LH, Manoukian SV, Cequier A, Lincoff MA, Rupprecht HJ, Gersh BJ, Mann T, Bertrand ME, Mehran R, Stone GW. Choice of arterial access site and outcomes in patients with acute coronary syndromes managed with an early invasive strategy: the ACUITY trial. EuroIntervention. 2009;5:115–120. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
