

Multi-modal imaging of adhesive capsulitis of the shoulder
- PMID: 27107871
- PMCID: PMC4877356
- DOI: 10.1007/s13244-016-0491-8
Multi-modal imaging of adhesive capsulitis of the shoulder
Abstract
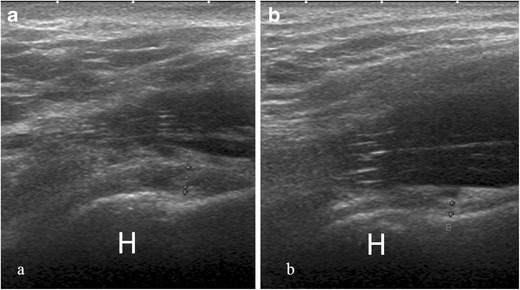
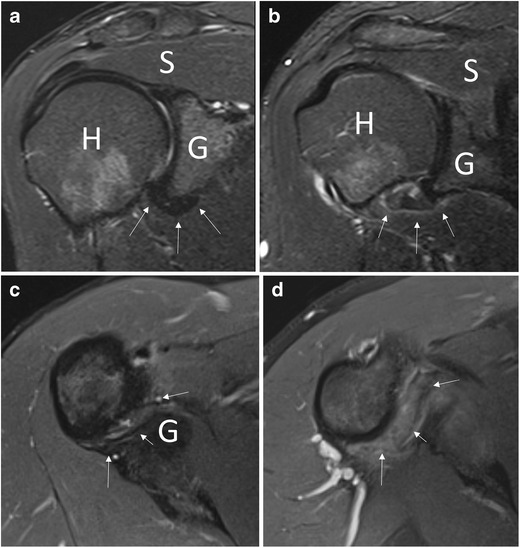
Adhesive capsulitis of the shoulder is a clinical condition characterized by progressive limitation of active and passive mobility of the glenohumeral joint, generally associated with high levels of pain. Although the diagnosis of adhesive capsulitis is based mainly on clinical examination, different imaging modalities including arthrography, ultrasound, magnetic resonance, and magnetic resonance arthrography may help to confirm the diagnosis, detecting a number of findings such as capsular and coracohumeral ligament thickening, poor capsular distension, extracapsular contrast leakage, and synovial hypertrophy and scar tissue formation at the rotator interval. Ultrasound can also be used to guide intra- and periarticular procedures for treating patients with adhesive capsulitis.
Key points: • Diagnosis of adhesive capsulitis is mainly based on clinical findings. • Imaging may be used to exclude articular or rotator cuff pathology. • Thickening of coracohumeral and inferior glenohumeral ligaments are common findings. • Rotator interval fat pad obliteration has 100 % specificity for adhesive capsulitis. • Ultrasound can be used to guide intra- and periarticular treatments.
Keywords: Adhesive capsulitis; Arthrography; Magnetic resonance; Shoulder; Ultrasound.
Figures








References
-
- Codman EA (1934) Rupture of the supraspinatus tendon and other lesions in or about the subacromial bursa. In: The shoulder. Privately printed, Boston. pp 216-224
-
- Neviaser JS. Adhesive capsulitis of the shoulder (the frozen shoulder) Med Times. 1962;90:783–780. - PubMed
-
- Sung CM, Jung TS, Park HB (2014) Are serum lipids involved in primary frozen shoulder? A case-control study. J Bone Joint Surg Am 96(21):1828–18s33 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
