

Vitamin K prophylaxis for prevention of vitamin K deficiency bleeding: a systematic review
- PMID: 27109090
- PMCID: PMC4862383
- DOI: 10.1038/jp.2016.30
Vitamin K prophylaxis for prevention of vitamin K deficiency bleeding: a systematic review
Abstract
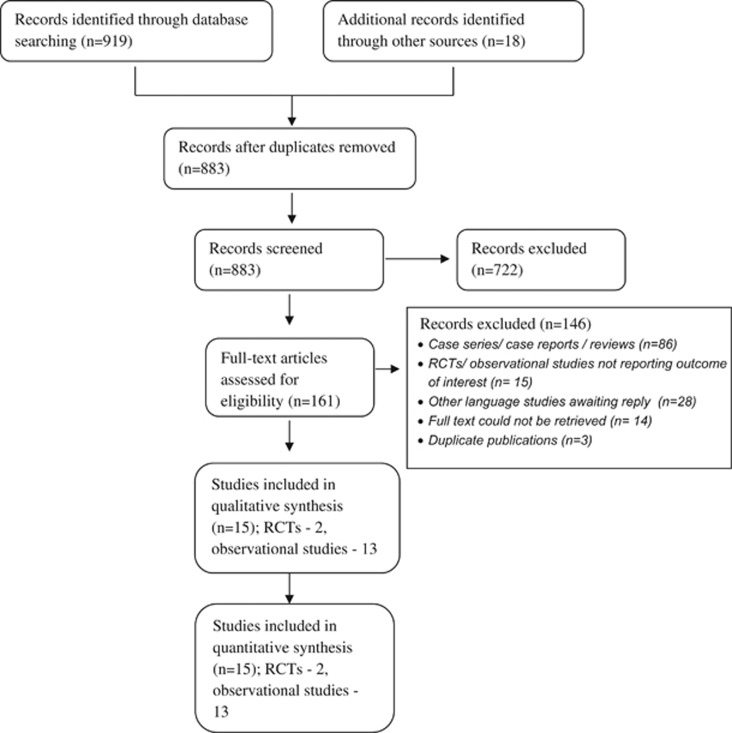
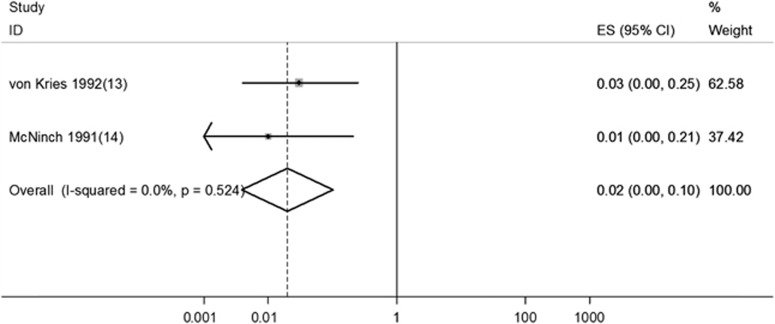
We conducted a systematic review to evaluate the burden of late vitamin K deficiency bleeding (VKDB) and the effect of vitamin K prophylaxis on the incidence of VKDB. We searched MEDLINE and other electronic databases, and included all observational studies including population surveys as well as randomized controlled trials (RCT). The median (interquartile range) burden of late VKDB was 35 (10.5 to 80) per 100 000 live births in infants who had not received prophylaxis at birth; the burden was much higher in low- and middle-income countries as compared with high-income countries-80 (72 to 80) vs 8.8 (5.8 to 17.8) per 100 000 live births. Two randomized trials evaluated the effect of intramuscular (IM) prophylaxis on the risk of classical VKDB. Although one trial reported a significant reduction in the incidence of any bleeding (relative risk (RR) 0.73, 95% confidence interval (CI) 0.56 to 0.96) and moderate to severe bleeding (RR 0.19, 0.08 to 0.46; number needed to treat (NNT) 74, 47 to 177), the other trial demonstrated a significant reduction in the risk of secondary bleeding after circumcision in male neonates (RR 0.18, CI 0.08 to 0.42; NNT 9, 6 to 15). No RCTs evaluated the effect of vitamin K prophylaxis on late VKDB. Data from four surveillance studies indicate that the use of IM/subcutaneous vitamin K prophylaxis could significantly reduce the risk of late VKDB when compared with no prophylaxis (pooled RR 0.02; 95% CI 0.00 to 0.10). When compared with IM prophylaxis, a single oral dose of vitamin K increased the risk of VKDB (RR 24.5; 95% CI 7.4 to 81.0) but multiple oral doses did not (RR 3.64; CI 0.82 to 16.3). There is low-quality evidence from observational studies that routine IM administration of 1 mg of vitamin K at birth reduces the incidence of late VKDB during infancy. Given the high risk of mortality and morbidity in infants with late VKDB, it seems appropriate to administer IM vitamin K prophylaxis to all neonates at birth. Future studies should compare the efficacy and safety of multiple oral doses with IM vitamin K and also evaluate the optimal dose of vitamin K in preterm neonates.
Figures
References
-
- Shearer MJ. Vitamin K metabolism and nutriture. Blood Rev 1992; 6(2): 92–104. - PubMed
-
- Van Hasselt PM, de Koning TJ, Kvist N, de Vries E, Lundin CR, Berger R et al. Prevention of vitamin K deficiency bleeding in breastfed infants: lessons from the Dutch and Danish biliary atresia registries. Pediatrics 2008; 121(4): e857–e863. - PubMed
-
- Widdershoven J, Lambert W, Motohara K, Monnens L, de Leenheer A, Matsuda I et al. Plasma concentrations of vitamin K1 and PIVKA-II in bottle-fed and breast-fed infants with and without vitamin K prophylaxis at birth. Eur J Pediatr 1988; 148(2):139–142. - PubMed
-
- Sutor AH. Vitamin K deficiency bleeding in infants and children. Semin Thromb Hemost 1995; 21: 317–329. - PubMed
-
- Lehmann J. Vitamin K as a prophylactic in 13,000 babies. Lancet 1944; i: 493–494.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
