

Time Course of Macular and Peripapillary Inner Retinal Thickness in Non-arteritic Anterior Ischaemic Optic Neuropathy Using Spectral-Domain Optical Coherence Tomography
- PMID: 27110047
- PMCID: PMC4819921
- DOI: 10.3109/01658107.2015.1136654
Time Course of Macular and Peripapillary Inner Retinal Thickness in Non-arteritic Anterior Ischaemic Optic Neuropathy Using Spectral-Domain Optical Coherence Tomography
Abstract
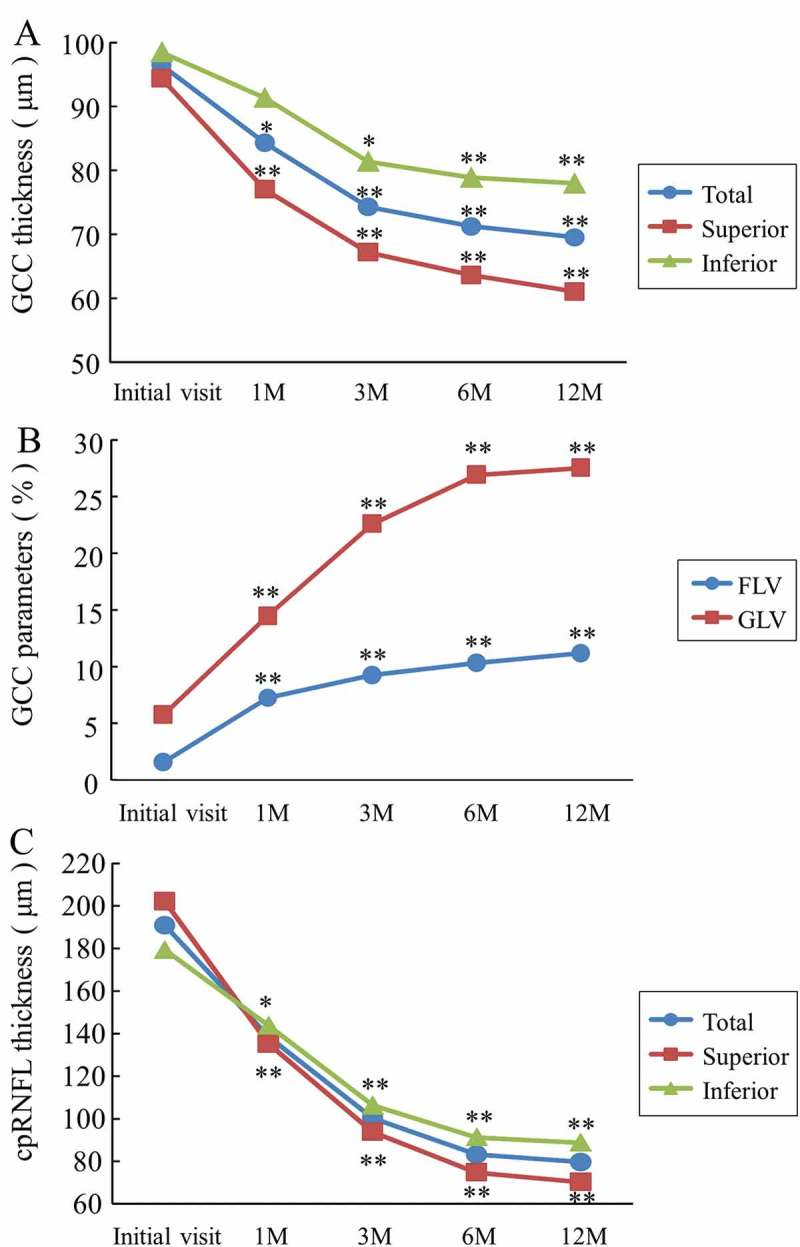
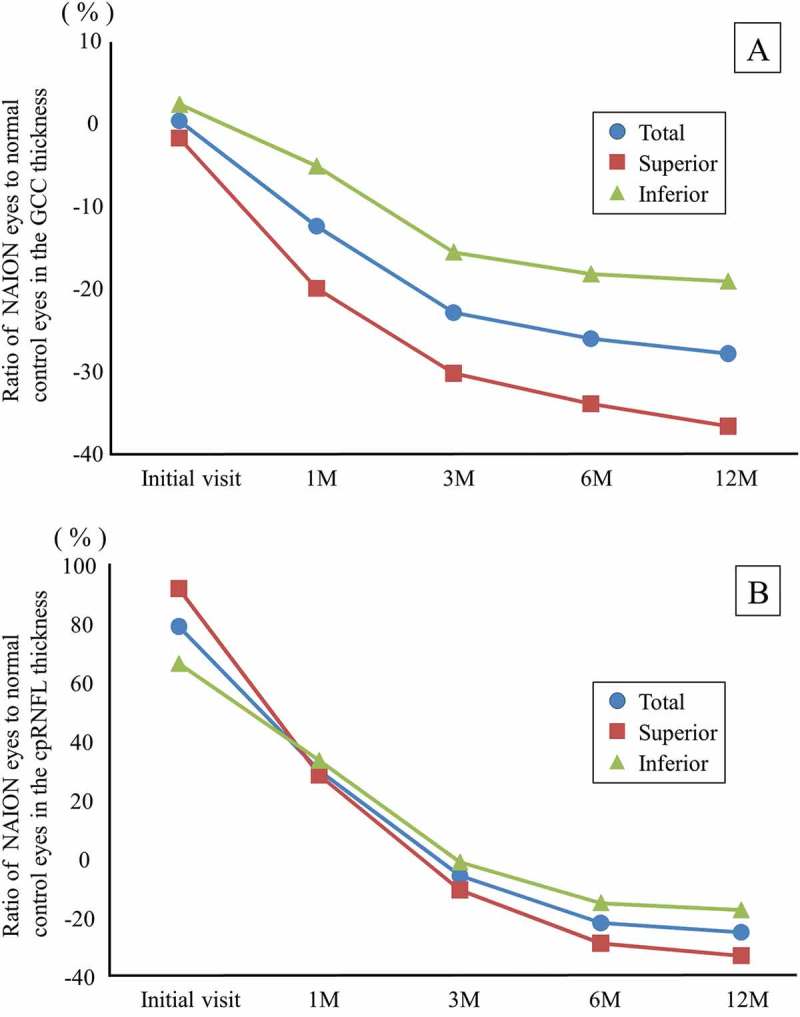
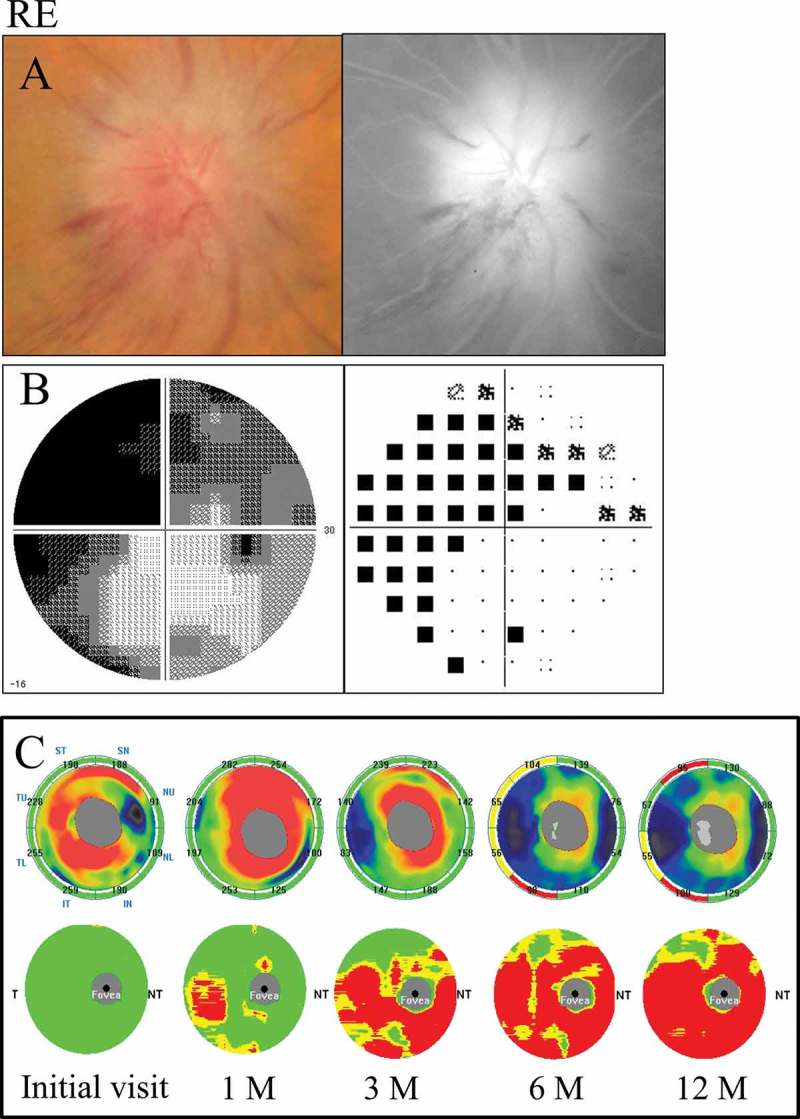
To report a time course of the ganglion cell complex (GCC) and circumpapillary retinal nerve fibre layer (cpRNFL) thicknesses using spectral-domain optical coherence tomography in patients with non-arteritic anterior ischaemic optic neuropathy (NAION), five patients with unilateral NAION were studied (the average age of 66.8 ± 7.8 years old). Forty-one age-matched normal controls were also enrolled. The GCC and cpRNFL thicknesses were measured at the initial visit and at 1, 3, 6, and 12 months using RTVue-100. The GCC thickness and the cpRNFL thickness of the patients were compared with those of the normal controls. The GCC thickness in the NAION patients was 96.49 μm at the initial visit, 84.28 μm at 1 month, 74.26 μm at 3 months, 71.23 μm at 6 months, and 69.51 μm at 12 months. The values at 1, 3, 6, and 12 months were significantly reduced (p < 0.01). The cpRNFL thickness at the initial visit was significantly increased, whereas the values at 6 and 12 months were significantly reduced (p < 0.01). The GCC thickness is more useful for the detection of retinal ganglion cell loss at an early stage than the cpRNFL thickness, because the GCC thickness is unaffected by optic disc swelling at the initial visit, unlike the cpRNFL thickness.
Keywords: Anterior ischaemic optic neuropathy; ganglion cell complex; retinal ganglion cell; retinal nerve fibre layer; spectral-domain optical coherence tomography.
Figures
References
-
- Hattenhauer MG, Leavitt JA, Hodge DO, Grill R, Gray DT.. Incidence of nonarteritic anterior ischemic optic neuropathy. Am J Ophthalmol 1997;123:103–107. - PubMed
-
- Hayreh SS, Zimmerman B.. Visual field abnormalities in nonarteritic anterior ischemic optic neuropathy: their pattern and prevalence at initial examination. Arch Ophthalmol 2005;123:1554–1562. - PubMed
-
- Gerling J, Meyer JH, Kommerell G.. Visual field defects in optic neuritis and anterior ischemic optic neuropathy: distinctive features. Graefes Arch Clin Exp Ophthalmol 1998;236:188–192. - PubMed
-
- Beck RW, Servais GE, Hayreh SS.. Anterior ischemic optic neuropathy. IX. Cup-to-disc ratio and its role in pathogenesis. Ophthalmology 1987;94:1503–1508. - PubMed
-
- Jonas JB, Xu L.. Optic disc morphology in eyes after nonarteritic anterior ischemic optic neuropathy. Invest Ophthalmol Vis Sci 1993;34:2260–2265. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources