

Clinical management of achalasia: current state of the art
- PMID: 27110134
- PMCID: PMC4831602
- DOI: 10.2147/CEG.S84019
Clinical management of achalasia: current state of the art
Abstract
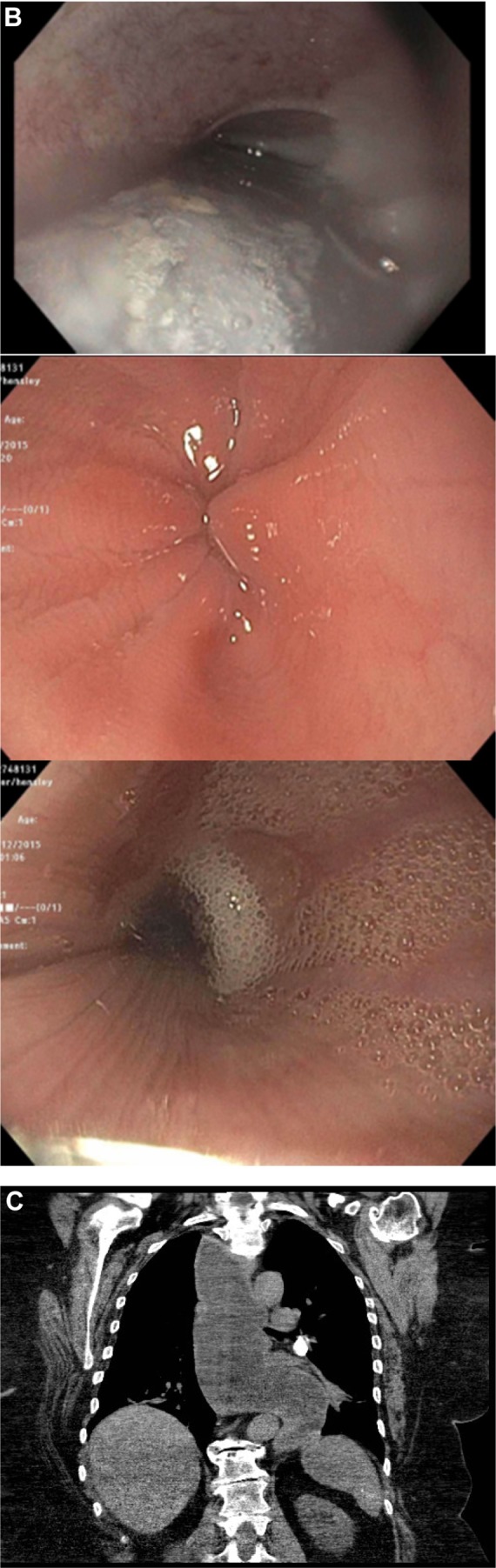
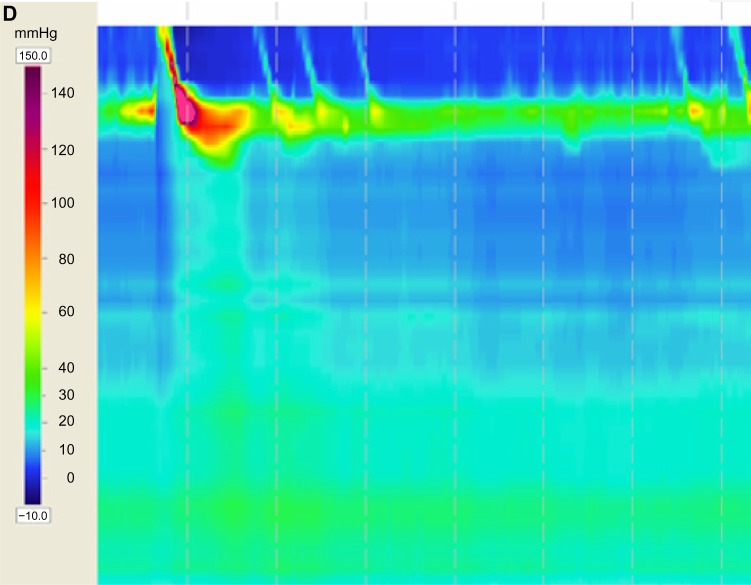
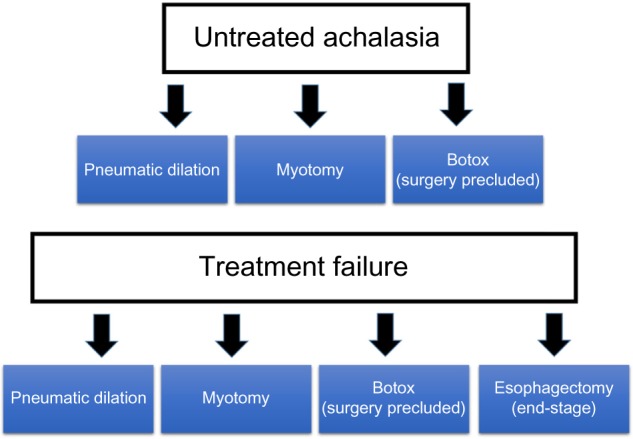
Achalasia is a primary disorder of esophageal motility. It classically presents with dysphagia to both solids and liquids but may be accompanied by regurgitation and chest pain. The gold standard for the diagnosis of achalasia is esophageal motility testing with manometry, which often reveals aperistalsis of the esophageal body and incomplete lower esophageal sphincter relaxation. The diagnosis is aided by complimentary tests, such as esophagogastroduodenoscopy and contrast radiography. Esophagogastroduodenoscopy is indicated to rule out mimickers of the disease known as "pseudoachalasia" (eg, malignancy). Endoscopic appearance of a dilated esophagus with retained food or saliva and a puckered lower esophageal sphincter should raise suspicion for achalasia. Additionally, barium esophagography may reveal a dilated esophagus with a distal tapering giving it a "bird's beak" appearance. Multiple therapeutic modalities aid in the management of achalasia, the decision of which depends on operative risk factors. Conventional treatments include medical therapy, botulinum toxin injection, pneumatic dilation, and Heller myotomy. The last two are defined as the most definitive treatment options. New emerging therapies include peroral endoscopic myotomy, placement of self-expanding metallic stents, and endoscopic sclerotherapy.
Keywords: Heller myotomy; achalasia; botulinum toxin injection; peroral endoscopic myotomy; pneumatic dilation; pseudoachalasia.
Figures

References
-
- Vaezi MF, Pandolfino JE, Vela MF. ACG clinical guideline: diagnosis and management of achalasia. Am J Gastroenterol. 2013;108(8):1238–1249. quiz 1250. - PubMed
-
- Clark SB, Rice TW, Tubbs RR, Richter JE, Goldblum JR. The nature of the myenteric infiltrate in achalasia: an immunohistochemical analysis. Am J Surg Pathol. 2000;24(8):1153–1158. - PubMed
-
- Richter JE. The diagnosis and misdiagnosis of achalasia: it does not have to be so difficult. Clin Gastroenterol Hepatol. 2011;9(12):1010–1011. - PubMed
-
- Kessing BF, Bredenoord AJ, Smout AJ. Erroneous diagnosis of gastroesophageal reflux disease in achalasia. Clin Gastroenterol Hepatol. 2011;9(12):1020–1024. - PubMed
-
- Vaezi MF, Richter JE. Diagnosis and management of achalasia. American College of Gastroenterology Practice Parameter Committee. Am J Gastroenterol. 1999;94(12):3406–3412. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
