

Obesogenic memory can confer long-term increases in adipose tissue but not liver inflammation and insulin resistance after weight loss
- PMID: 27110485
- PMCID: PMC4837291
- DOI: 10.1016/j.molmet.2015.12.001
Obesogenic memory can confer long-term increases in adipose tissue but not liver inflammation and insulin resistance after weight loss
Abstract
Objective: Obesity represents a major risk factor for the development of type 2 diabetes mellitus, atherosclerosis and certain cancer entities. Treatment of obesity is hindered by the long-term maintenance of initially reduced body weight, and it remains unclear whether all pathologies associated with obesity are fully reversible even upon successfully maintained weight loss.
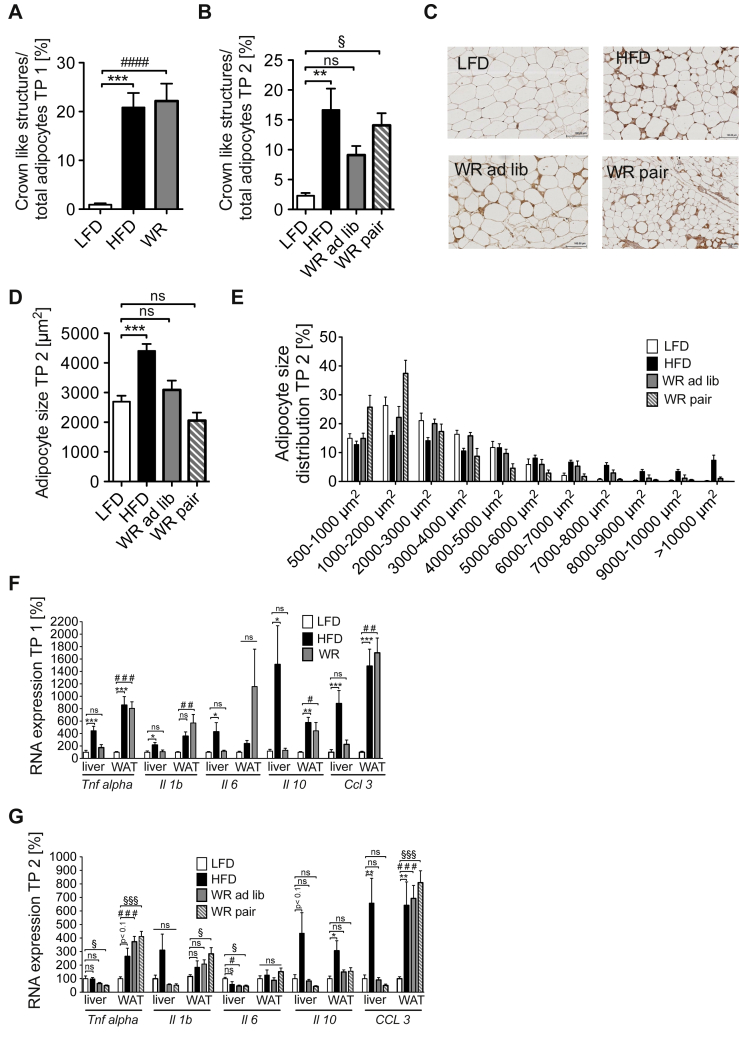
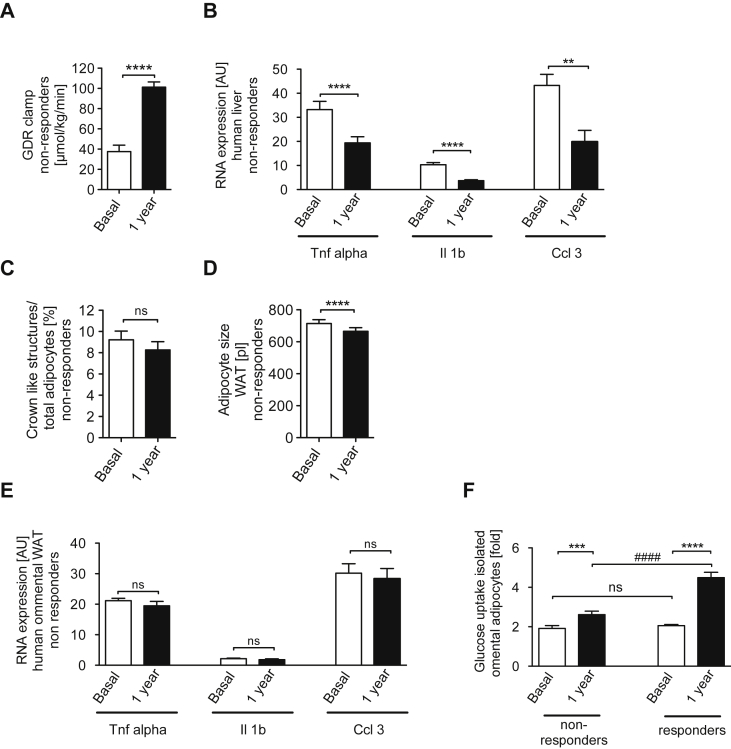
Methods: We compared high fat diet-fed, weight reduced and lean mice in terms of body weight development, adipose tissue and liver insulin sensitivity as well as inflammatory gene expression. Moreover, we assessed similar parameters in a human cohort before and after bariatric surgery.
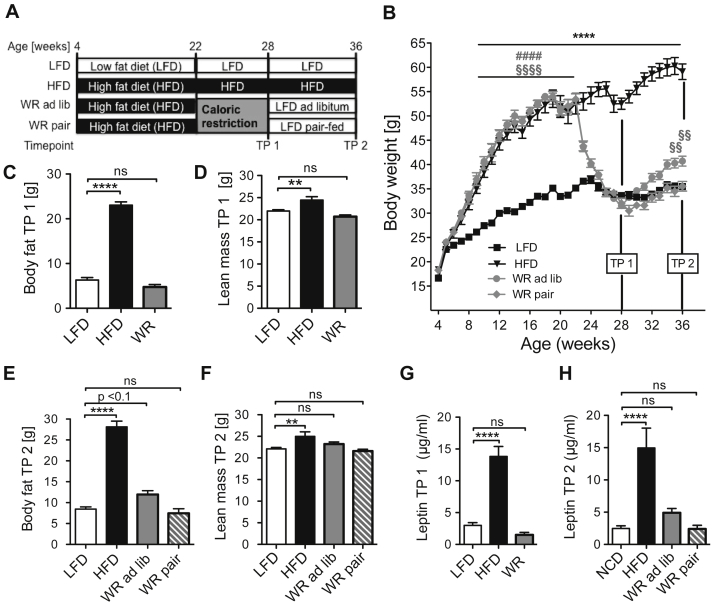
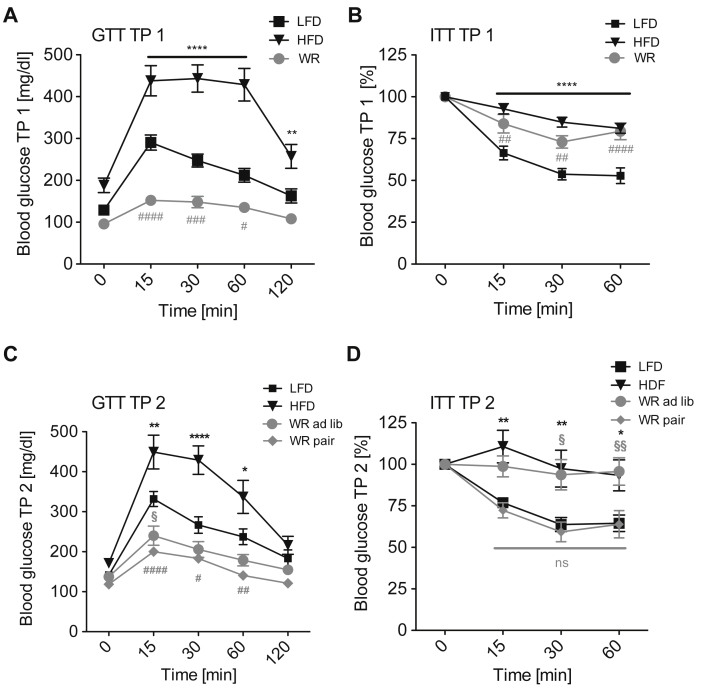
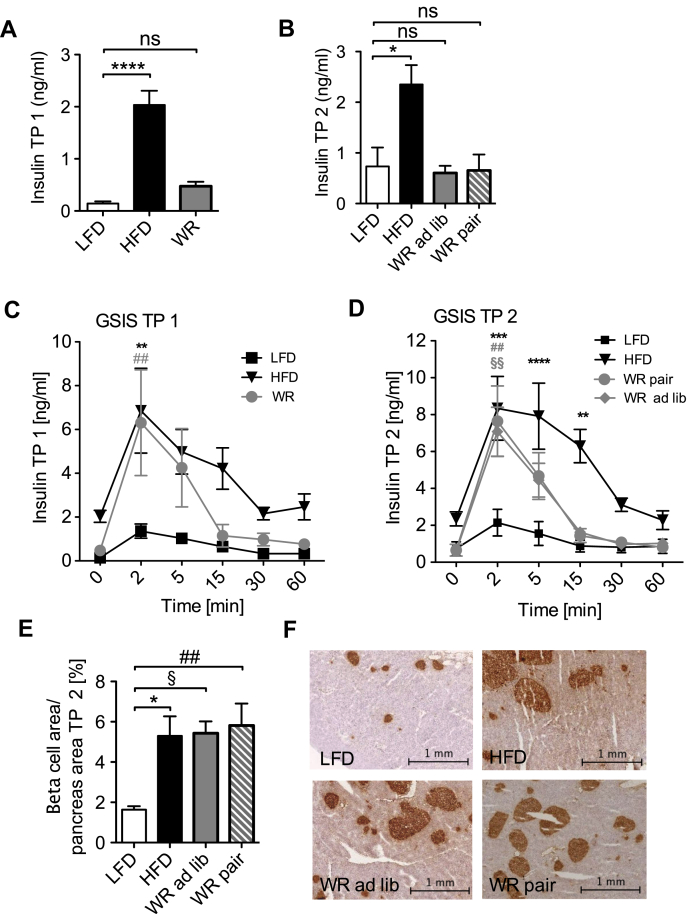
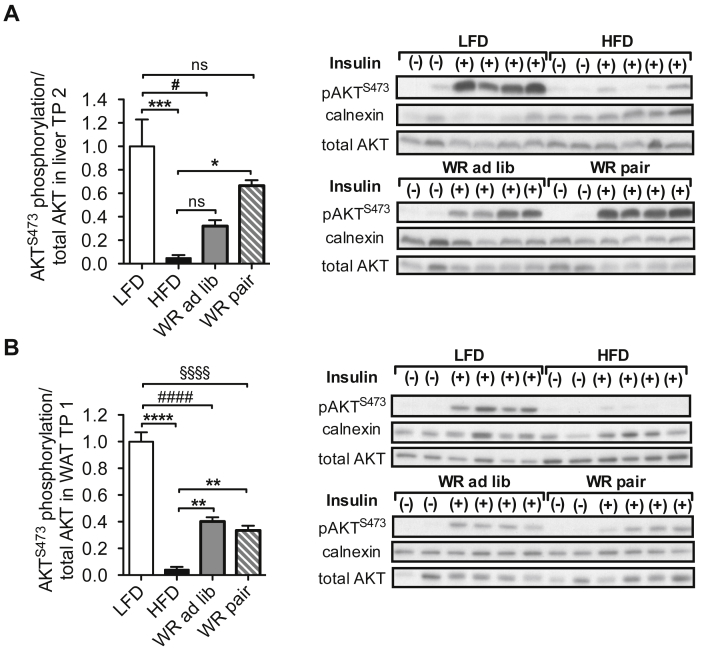
Results: Compared to lean animals, mice that demonstrated successful weight reduction showed increased weight gain following exposure to ad libitum control diet. However, pair-feeding weight-reduced mice with lean controls efficiently stabilized body weight, indicating that hyperphagia was the predominant cause for the observed weight regain. Additionally, whereas glucose tolerance improved rapidly after weight loss, systemic insulin resistance was retained and ameliorated only upon prolonged pair-feeding. Weight loss enhanced insulin action and resolved pro-inflammatory gene expression exclusively in the liver, whereas visceral adipose tissue displayed no significant improvement of metabolic and inflammatory parameters compared to obese mice. Similarly, bariatric surgery in humans (n = 55) resulted in massive weight reduction, improved hepatic inflammation and systemic glucose homeostasis, while adipose tissue inflammation remained unaffected and adipocyte-autonomous insulin action only exhibit minor improvements in a subgroup of patients (42%).
Conclusions: These results demonstrate that although sustained weight loss improves systemic glucose homeostasis, primarily through improved inflammation and insulin action in liver, a remarkable obesogenic memory can confer long-term increases in adipose tissue inflammation and insulin resistance in mice as well as in a significant subpopulation of obese patients.
Keywords: Insulin resistance; Metabolic inflammation; Obesity; Weight loss; Weight regain.
Figures
References
-
- Finucane M.M., Stevens G.A., Cowan M.J., Danaei G., Lin J.K., Paciorek C.J. National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9·1 million participants. Lancet. 2011;377:557–567. - PMC - PubMed
-
- W.H. Organisation, http://www.who.int/mediacentre/factsheets/fs311/en/index.html, 2013 (n.d.).
-
- Flegal K.M., Graubard B.I., Williamson D.F., Gail M.H. Cause-specific excess deaths associated with underweight, overweight, and obesity. Journal of American of Medical Association. 2007;298:2028–2037. - PubMed
-
- Leblanc E.S., O'Connor E., Whitlock E.P., Patnode C.D., Kapka T. Effectiveness of primary care-relevant treatments for obesity in adults: a systematic evidence review for the U.S. Preventive Services Task Force. Annals of Internal Medicine. 2011;155:434–447. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
