

Early Blood Pressure Reduction in Acute Ischemic Stroke with Various Severities: A Subgroup Analysis of the CATIS Trial
- PMID: 27110711
- PMCID: PMC8784237
- DOI: 10.1159/000444722
Early Blood Pressure Reduction in Acute Ischemic Stroke with Various Severities: A Subgroup Analysis of the CATIS Trial
Abstract
Background: Clinical trials have generally showed a neutral effect of blood pressure (BP) reduction on clinical outcomes among acute ischemic stroke patients. We conducted a prespecified subgroup analysis to assess whether disease severity modifies the effect of early antihypertensive treatment on death and disability among patients with acute ischemic stroke.
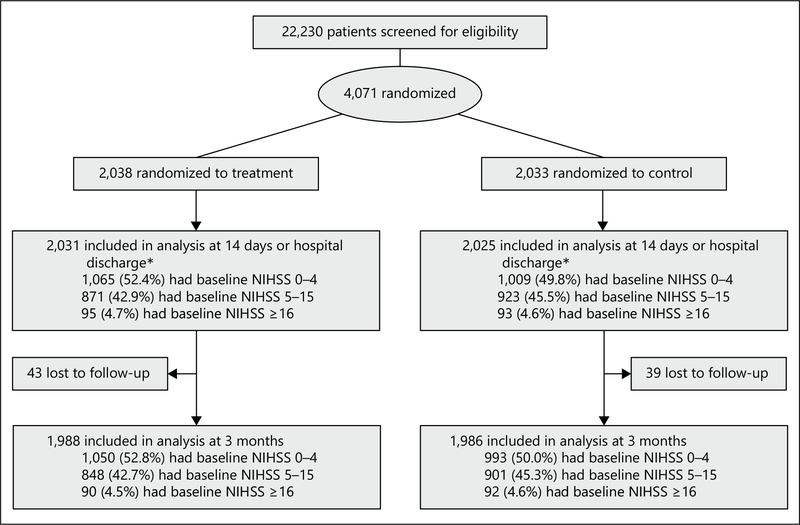
Methods: In the China Antihypertensive Trial in Acute Ischemic Stroke, 4,071 patients with acute ischemic stroke and elevated BP were randomly assigned to receive antihypertensive treatment or to discontinue all hypertension medications within 48 h of symptom onset. The primary outcome was a combination of death and major disability at 14 days or hospital discharge. In this subgroup analysis, participants were categorized into 3 groups according to their baseline NIH Stroke Scale (NIHSS) scores (0-4, 5-15, or ≥16).
Results: At 24 h after randomization, mean systolic BP differences (95% CIs) were -8.5 (-10.0 to -7.1), -9.8 (-11.4 to -8.3), and -9.1 (-14.4 to -3.8) mm Hg between the treatment and control groups (all p values <0.001) for patients with a baseline NIHSS score of 0-4, 5-15, and ≥16, respectively. At day 7 after randomization, the corresponding mean systolic BP differences were -9.3 (-10.5 to -8.2), -9.1 (-10.3 to -7.8), and -10.1 (-15.1 to -5.1) mm Hg between the treatment and control groups (all p values <0.001). The primary outcome was not significantly different between the treatment and control groups at day 14 or hospital discharge among all NIHSS subgroups (p value for homogeneity = 0.66). ORs (95% CI) associated with treatment were 1.14 (0.87-1.49, p = 0.33), 1.04 (0.86-1.25, p = 0.70), and 0.67 (0.18-2.44, p = 0.54) for patients with a baseline NIHSS score of 0-4, 5-15, and ≥16, respectively. The composite outcome of death and major disability at 3-month follow-up did not differ between the 2 comparison groups for all NIHSS subgroups. In addition, vascular events and recurrent stroke were not significantly different between the 2 comparison groups at the 3-month follow-up visit among all NIHSS subgroups except that there was a suggestive risk reduction for recurrent stroke among those with an NIHSS score of 5-15 (OR 0.45, 95% CI 0.20-0.99, p = 0.05).
Conclusion: Early BP reduction with antihypertensive medications did not reduce or increase the risk of death, major disabilities, recurrent instances of stroke, and vascular events in acute ischemic stroke patients with a variety of disease severities.
© 2016 S. Karger AG, Basel.
Figures
Similar articles
-
Effects of immediate blood pressure reduction on death and major disability in patients with acute ischemic stroke: the CATIS randomized clinical trial.JAMA. 2014 Feb 5;311(5):479-89. doi: 10.1001/jama.2013.282543. JAMA. 2014. PMID: 24240777 Clinical Trial.
-
Immediate Antihypertensive Treatment for Patients With Acute Ischemic Stroke With or Without History of Hypertension: A Secondary Analysis of the CATIS Randomized Clinical Trial.JAMA Netw Open. 2019 Jul 3;2(7):e198103. doi: 10.1001/jamanetworkopen.2019.8103. JAMA Netw Open. 2019. PMID: 31365109 Free PMC article. Clinical Trial.
-
Early Versus Delayed Antihypertensive Treatment After Acute Ischemic Stroke by Hypertension History.Stroke. 2025 Mar;56(3):631-639. doi: 10.1161/STROKEAHA.124.049242. Epub 2025 Jan 14. Stroke. 2025. PMID: 39807580 Clinical Trial.
-
The management of hypertension for an acute stroke: what is the blood pressure goal?Curr Cardiol Rep. 2013 Jun;15(6):366. doi: 10.1007/s11886-013-0366-2. Curr Cardiol Rep. 2013. PMID: 23605468 Review.
-
Effect of Pretreatment Blood Pressure on Outcomes in Thrombolysed Acute Ischemic Stroke Patients: A Systematic Review and Meta-analysis.J Stroke Cerebrovasc Dis. 2019 Apr;28(4):906-919. doi: 10.1016/j.jstrokecerebrovasdis.2018.12.008. Epub 2019 Jan 3. J Stroke Cerebrovasc Dis. 2019. PMID: 30612890
Cited by
-
Application of 3.0T magnetic resonance arterial spin labeling (ASL) technology in mild and moderate intracranial atherosclerotic stenosis.Exp Ther Med. 2016 Jul;12(1):297-301. doi: 10.3892/etm.2016.3318. Epub 2016 May 9. Exp Ther Med. 2016. PMID: 27347052 Free PMC article.
-
Triiodothyronine levels were positively correlated with opening of collateral circulation in cerebral infarction patients with large artery atherosclerosis.Arch Med Sci. 2019 Dec 31;16(1):51-57. doi: 10.5114/aoms.2020.91286. eCollection 2020. Arch Med Sci. 2019. PMID: 32051705 Free PMC article.
-
Effect of General Anesthesia vs. Conscious Sedation on the Outcomes of Acute Ischemic Stroke Patients After Endovascular Therapy: A Meta-Analysis of Randomized Clinical Trials.Front Neurol. 2019 Oct 31;10:1131. doi: 10.3389/fneur.2019.01131. eCollection 2019. Front Neurol. 2019. PMID: 31736853 Free PMC article.
-
Early antihypertensive treatment and clinical outcomes in acute ischemic stroke: subgroup analysis by baseline blood pressure.J Hypertens. 2018 Jun;36(6):1372-1381. doi: 10.1097/HJH.0000000000001690. J Hypertens. 2018. PMID: 29389742 Free PMC article. Clinical Trial.
-
2022 Guidelines of the Taiwan Society of Cardiology and the Taiwan Hypertension Society for the Management of Hypertension.Acta Cardiol Sin. 2022 May;38(3):225-325. doi: 10.6515/ACS.202205_38(3).20220321A. Acta Cardiol Sin. 2022. PMID: 35673334 Free PMC article.
References
-
- Wang Y, Xu J, Zhao X, Wang D, Wang C, Liu L, Wang A, Meng X, Li H, Wang Y: Association of hypertension with stroke recurrence depends on ischemic stroke subtype. Stroke 2013;44:1232–1237. - PubMed
-
- Carlberg B, Asplund K, Hägg E: Factors influencing admission blood pressure levels in patients with acute stroke. Stroke 1991;22:527–530. - PubMed
-
- Qureshi AI: Acute hypertensive response in patients with stroke: pathophysiology and management. Circulation 2008;118:176–187. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
