

Quantifying Temporomandibular Joint Synovitis in Children With Juvenile Idiopathic Arthritis
- PMID: 27110936
- PMCID: PMC5573997
- DOI: 10.1002/acr.22911
Quantifying Temporomandibular Joint Synovitis in Children With Juvenile Idiopathic Arthritis
Abstract
Objective: Juvenile idiopathic arthritis (JIA) frequently affects the temporomandibular joints (TMJs) and is often undetected by history, examination, and plain imaging. Qualitative assessment of gadolinium-enhanced magnetic resonance images (MRIs) is currently the standard for diagnosis of TMJ synovitis associated with JIA. The purpose of this study is to apply a quantitative analysis of synovial enhancement to MRIs of patients with and without JIA to establish a disease threshold and sensitivity and specificity for the technique.
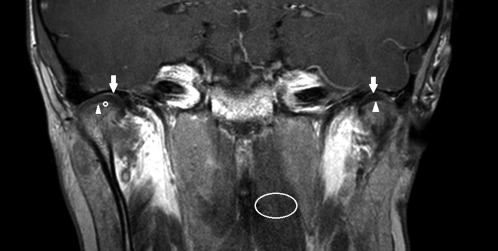
Methods: This is a retrospective case-control study of children (age ≤16 years) who had MRIs with gadolinium including the TMJs. Subjects were divided into a JIA group and a control group. From a coronal T1-weighted image, a ratio (enhancement ratio [ER]) of the average pixel intensity within three 0.2-mm2 regions of interest (ROIs) in the TMJ synovium to that of a 50-mm2 ROI of the longus capitis muscle was calculated. Receiver operating characteristic curves were used to determine the sensitivity and specificity. The inter- and intraexaminer reliability was evaluated with Bland-Altman plots and 2-way mixed, absolute agreement intraclass correlation coefficients.
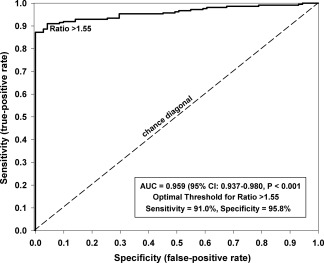
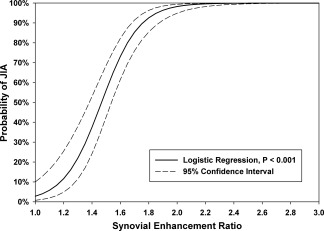
Results: There were 187 and 142 TMJs included in the JIA and control groups, respectively. An ER threshold of 1.55 had a sensitivity and specificity for detecting synovitis of 91% and 96%, respectively. The inter- and intraexaminer reliability was excellent.
Conclusion: Calculating a ratio of pixel intensity between the TMJ synovium and the longus capitis muscle is a reliable way to quantify synovial enhancement. An ER of 1.55 differentiates normal TMJs from those affected by inflammatory arthritis.
© 2016, American College of Rheumatology.
Figures

Similar articles
-
Quantifying the Effect of Temporomandibular Joint Intra-Articular Steroid Injection on Synovial Enhancement in Juvenile Idiopathic Arthritis.J Oral Maxillofac Surg. 2016 Dec;74(12):2363-2369. doi: 10.1016/j.joms.2016.06.189. Epub 2016 Jul 5. J Oral Maxillofac Surg. 2016. PMID: 27474460
-
Optimization of Quantitative Dynamic Postgadolinium MRI Technique Using Normalized Ratios for the Evaluation of Temporomandibular Joint Synovitis in Patients with Juvenile Idiopathic Arthritis.AJNR Am J Neuroradiol. 2017 Dec;38(12):2344-2350. doi: 10.3174/ajnr.A5424. Epub 2017 Nov 23. AJNR Am J Neuroradiol. 2017. PMID: 29170273 Free PMC article.
-
Quantifying Synovial Enhancement of the Pediatric Temporomandibular Joint.J Oral Maxillofac Surg. 2016 Oct;74(10):1937-45. doi: 10.1016/j.joms.2016.03.010. Epub 2016 Mar 21. J Oral Maxillofac Surg. 2016. PMID: 27067062
-
Imaging of temporomandibular joint abnormalities in juvenile idiopathic arthritis with a focus on developing a magnetic resonance imaging protocol.Pediatr Radiol. 2018 Jun;48(6):792-800. doi: 10.1007/s00247-017-4005-8. Epub 2018 May 8. Pediatr Radiol. 2018. PMID: 29766249 Review.
-
MRI of the temporomandibular joint in children with juvenile idiopathic arthritis: protocol and findings.Pediatr Radiol. 2023 Jul;53(8):1498-1512. doi: 10.1007/s00247-023-05616-7. Epub 2023 Mar 22. Pediatr Radiol. 2023. PMID: 36944679 Review.
Cited by
-
Contrast-enhanced MRI compared to direct joint visualization at arthroscopy in pediatric patients with suspected temporomandibular joint synovitis.Pediatr Radiol. 2019 Feb;49(2):196-202. doi: 10.1007/s00247-018-4291-9. Epub 2018 Oct 31. Pediatr Radiol. 2019. PMID: 30382321
-
Initial radiological signs of dentofacial deformity in juvenile idiopathic arthritis.Sci Rep. 2021 Jun 23;11(1):13142. doi: 10.1038/s41598-021-92575-4. Sci Rep. 2021. PMID: 34162967 Free PMC article.
-
The Diagnosis and Treatment of Rheumatoid and Juvenile Idiopathic Arthritis of the Temporomandibular Joint.Dtsch Arztebl Int. 2022 Jan 28;119(4):47-54. doi: 10.3238/arztebl.m2021.0388. Dtsch Arztebl Int. 2022. PMID: 34874262 Free PMC article.
-
Defining the normal appearance of the temporomandibular joints by magnetic resonance imaging with contrast: a comparative study of children with and without juvenile idiopathic arthritis.Pediatr Rheumatol Online J. 2018 Jan 24;16(1):8. doi: 10.1186/s12969-018-0223-3. Pediatr Rheumatol Online J. 2018. PMID: 29368603 Free PMC article.
-
Controversial Aspects of Diagnostics and Therapy of Arthritis of the Temporomandibular Joint in Rheumatoid and Juvenile Idiopathic Arthritis-An Analysis of Evidence- and Consensus-Based Recommendations Based on an Interdisciplinary Guideline Project.J Clin Med. 2022 Mar 22;11(7):1761. doi: 10.3390/jcm11071761. J Clin Med. 2022. PMID: 35407368 Free PMC article.
References
-
- Ringold S, Thapa M, Shaw EA, Wallace CA. Heterotopic ossification of the temporomandibular joint in juvenile idiopathic arthritis. J Rheumatol 2011;38:1423–8. - PubMed
-
- Cannizzaro E, Schroeder S, Muller LM, Kellenberger CJ, Saurenmann RK. Temporomandibular joint involvement in children with juvenile idiopathic arthritis. J Rheumatol 2011;38:510–5. - PubMed
-
- Stoll ML, Sharpe T, Beukelman T, Good J, Young D, Cron RQ. Risk factors for temporomandibular joint arthritis in children with juvenile idiopathic arthritis. J Rheumatol 2012;39:1880–7. - PubMed
-
- Twilt M, Mobers SM, Arends LR, ten Cate R, van Suijlekom‐Smit L. Temporomandibular involvement in juvenile idiopathic arthritis. J Rheumatol 2004;31:1418–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
