

Tinnitus Suppression by Intracochlear Electrical Stimulation in Single Sided Deafness - A Prospective Clinical Trial: Follow-Up
- PMID: 27111333
- PMCID: PMC4844154
- DOI: 10.1371/journal.pone.0153131
Tinnitus Suppression by Intracochlear Electrical Stimulation in Single Sided Deafness - A Prospective Clinical Trial: Follow-Up
Abstract
Introduction: Earlier studies show that a Cochlear Implant (CI), capable of providing intracochlear electrical stimulation independent of environmental sounds, appears to suppress tinnitus at least for minutes. The current main objective is to compare the long-term suppressive effects of looped (i.e. repeated) electrical stimulation (without environmental sound perception) with the standard stimulation pattern of a CI (with environmental sound perception). This could open new possibilities for the development of a "Tinnitus Implant" (TI), an intracochlear pulse generator for the suppression of tinnitus.
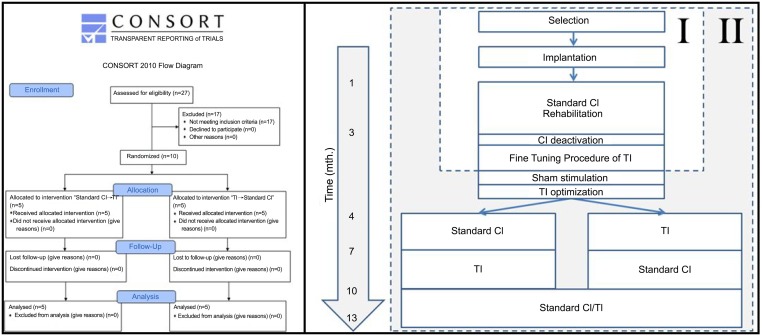
Materials and methods: Ten patients with single sided deafness suffering from unilateral tinnitus in the deaf ear are fitted with a CI (MED-EL Corporation, Innsbruck, Austria). Stimulation patterns are optimized for each individual patient, after which they are compared using a randomized crossover design, with a follow-up of six months, followed by a 3 month period using the modality of patient's choice.
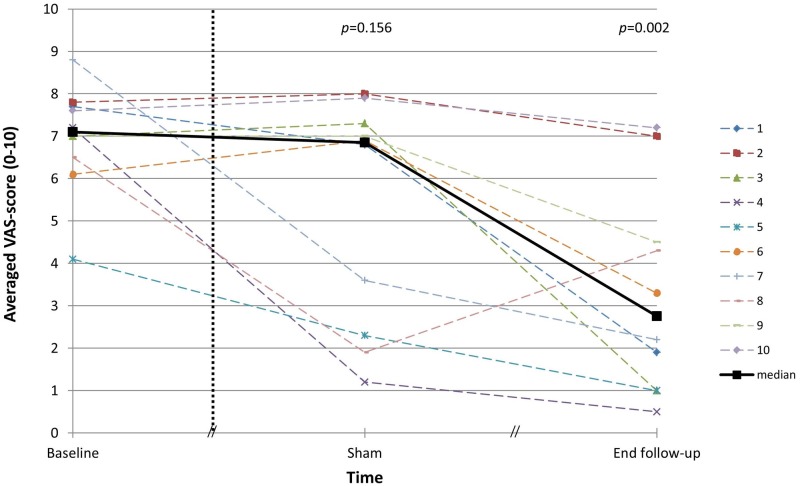
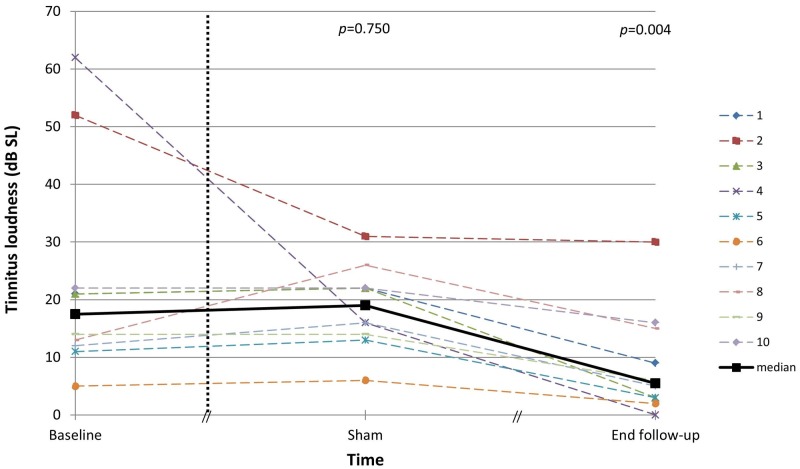
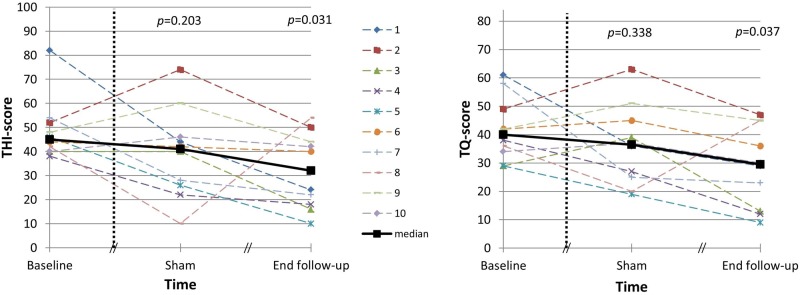
Results: Results show that tinnitus can be suppressed with intracochlear electrical stimulation independent of environmental sounds, even long term. No significant difference in tinnitus suppression was found between the standard clinical CI and the TI.
Conclusion: It can be concluded that coding of environmental sounds is no requirement for tinnitus suppression with intracochlear electrical stimulation. It is therefore plausible that tinnitus suppression by CI is not solely caused by an attention shift from the tinnitus to environmental sounds. Both the standard clinical CI and the experimental TI are potential treatment options for tinnitus. These findings offer perspectives for a successful clinical application of the TI, possibly even in patients with significant residual hearing.
Trial registration: TrialRegister.nl NTR3374.
Conflict of interest statement
Figures

References
-
- Heller MF, Bergman M. Tinnitus aurium in normally hearing persons. Ann Otol 1953; 62:73–83. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
