

Effects of acute hemorrhage on intrapulmonary shunt in a pig model of acute respiratory distress-like syndrome
- PMID: 27113037
- PMCID: PMC4845492
- DOI: 10.1186/s12890-016-0221-5
Effects of acute hemorrhage on intrapulmonary shunt in a pig model of acute respiratory distress-like syndrome
Abstract
Background: In acute respiratory distress syndrome (ARDS), gas exchange and respiratory system mechanics (compliance) are severely impaired. Besides ventilatory parameters, the degree of respiratory abnormality can be influenced by the circulatory state. This study investigated the influence of acute hypovolemia on the respiratory system.
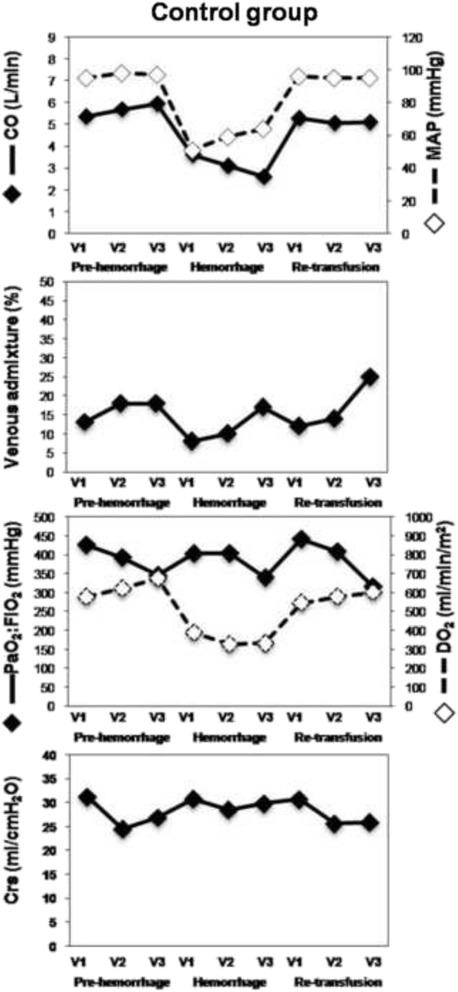
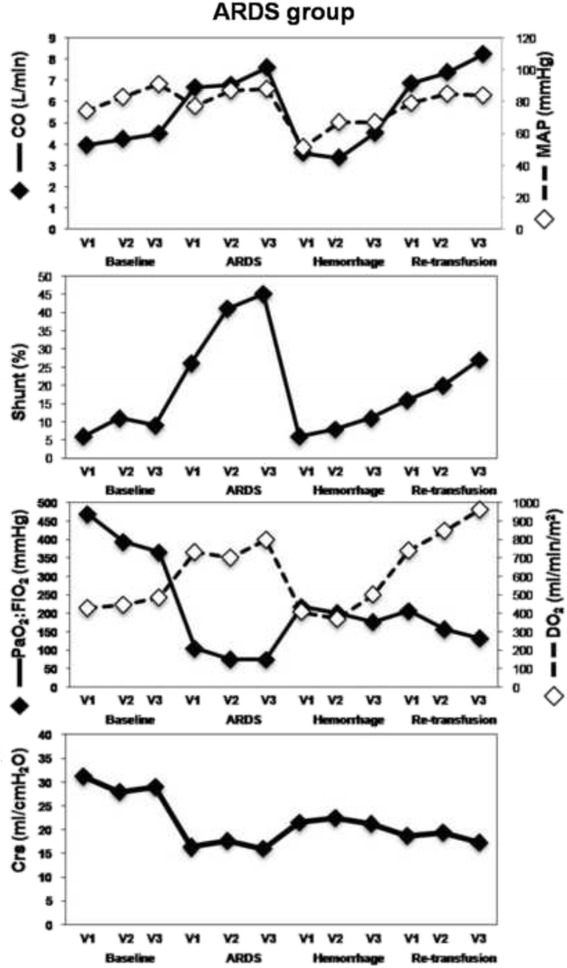
Methods: We performed a secondary analysis of a previous study including 8 pigs with ARDS-like syndrome induced by lung lavage and surfactant depletion method (ARDS group) and 10 mechanically ventilated pigs with no intervention (CTRL group). Animals of both groups were subjected to hemorrhage and retransfusion successively. We reanalyzed the effect of acute blood volume variations on intrapulmonary shunt (shunt), arterial oxygenation (PaO2:FiO2), global oxygen delivery (DO2) and respiratory system compliance (Crs).
Results: In the ARDS group, after hemorrhage, shunt decreased (-28 +/- 3.5 % (p < 0.001)), respiratory system compliance (Crs) increased (+5.1 +/- 1.0 ml/cm H2O (p < 0.001)) moreover, there was a concurrent increase in PaO2:FiO2 (+113 +/- 19.1 mmHg; p < 0.001) but this did not prevent a reduction in DO2 (-317 +/- 49.8 ml/min; p < 0.001). Following retransfusion, shunt and Crs return towards pre-hemorrhage values. Similar changes, but of smaller magnitude were observed in the CTRL group, except that no significant changes in oxygenation occurred.
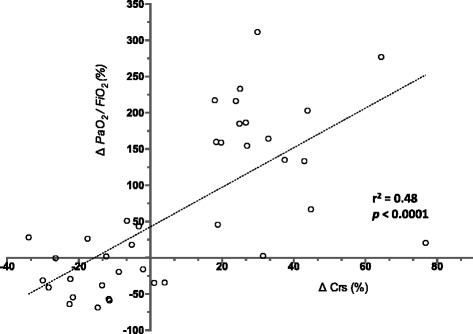
Conclusions: The present analysis suggests that an acute decrease in blood volume results in a decrease in shunt with a parallel improvement in arterial oxygenation and an increase in Crs during ARDS-like syndrome. Our results strengthen the importance to integrate the circulatory condition in the analysis of the state of the respiratory system. However, the translation of this physiological model in a clinical perspective is not straightforward because our model of acute and severe hemorrhage is not strictly equivalent to a progressive hypovolemia, as could be obtained in ICU by diuretic. Furthermore, the present model does not consider the impact of blood loss induced decrease of DO2 on other vital organs function.
Trial registration: 'Not applicable'.
Keywords: Admission; Lung compliance; Transpulmonary blood flow.
Figures
References
-
- Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342(18):1301–8. - PubMed
-
- Breen PH, Schumacker PT, Sandoval J, Mayers I, Oppenheimer L, Wood LD. Increased cardiac output increases shunt: role of pulmonary edema and perfusion. J Appl Physiol. 1985;59:1313–21. - PubMed
-
- Fulton RL, Fischer RP. Pulmonary changes due to hemorrhagic shock resuscitation with isotonic and hypertonic saline. Surgery. 1974;75:881–91. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
