

Surgical outcomes and complications of posterior hemivertebra resection in children younger than 5 years old
- PMID: 27113726
- PMCID: PMC4845311
- DOI: 10.1186/s13018-016-0381-2
Surgical outcomes and complications of posterior hemivertebra resection in children younger than 5 years old
Abstract
Background: There have been many reports on posterior hemivertebra resection. However, there were few articles in very young cases. This is a clinical retrospective study to evaluate the complications and efficacy of posterior hemivertebra resection in very young cases.
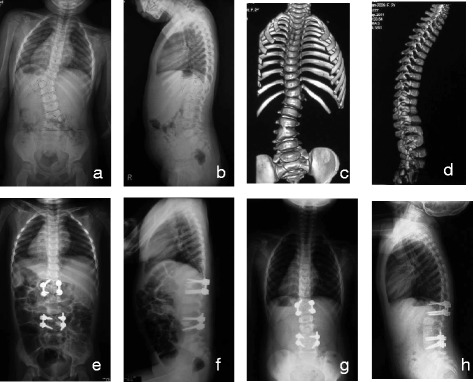
Methods: From January 2003 to January 2012, 39 consecutive cases of congenital scoliosis with hemivertebra were retrospectively investigated in our hospital, including 18 females and 21 males, aged from 21 to 65 months old (average 42.4 months). All the cases underwent posterior hemivertebra resection with transpedicular instrumentation. Clinical charts and radiographs of spine were retrospectively reviewed to record complications and outcomes postoperatively and at the latest follow-up.
Results: Mean operation time was 186.4 min (90-280 min) with average blood loss of 306.6 (100-700) ml. The total number of hemivertebrae resected was 43, including one hemivertebra in 35 cases and two hemivertebrae in 4 cases. The mean number of fused segments was 3.4, including 22 cases (56.4 %) with bisegmental fusion and 4 cases with mesh cage. Average follow-up period was 5.4 (3 to 11) years. There was a mean improvement rate of 83.6 % in the segmental scoliosis from 38.4° before surgery to 6.3° after operation and a mean improvement rate of 81.9 % in segmental kyphosis from 17.1° to 3.2° over the same time. The spontaneous correction rates of the compensatory cranial curve and compensatory caudal curve were 65.7 and 66.9 %, respectively. There were three complications (two cases),one pedicle fractures, one rod breakages, and one additional surgery for curve progression. Besides these, two additional surgeries (two cases) were performed to remove the instrumentation for pedicle elongation in the follow-up. There was no neurological complication.
Conclusions: Posterior hemivertebra resection with transpedicular instrumentation is a safe and effective procedure in very young congenital scoliosis cases. Earlier surgeries can achieve short fusion and save more mobile segments. However, complications associated with implants and spinal growth still remain major concerns.
Keywords: Complication; Congenital scoliosis; Hemivertebra resection; Posterior surgery; Surgical outcome.
Figures

References
-
- McMaster MJ, Ohtsuka K. The natural history of congenital scoliosis. A study of two hundred and fifty-one patients. J Bone Joint Surg Am. 1982;64(8):1128–47. - PubMed
-
- McMaster MJ, David CV. Hemivertebra as a cause of scoliosis. A study of 104 patients. J Bone Joint Surg Br. 1986;68(4):588–95. - PubMed
-
- Nasca RJ, Stilling FH, Stell HH. Progression of congenital scoliosis due to hemivertebrae and hemivertebrae with bars. J Bone Joint Surg Am. 1975;57(4):456–66. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
