

Atypical Clinical Presentation of Sporotrichosis Caused by Sporothrix globosa Resistant to Itraconazole
- PMID: 27114300
- PMCID: PMC4889737
- DOI: 10.4269/ajtmh.15-0267
Atypical Clinical Presentation of Sporotrichosis Caused by Sporothrix globosa Resistant to Itraconazole
Abstract
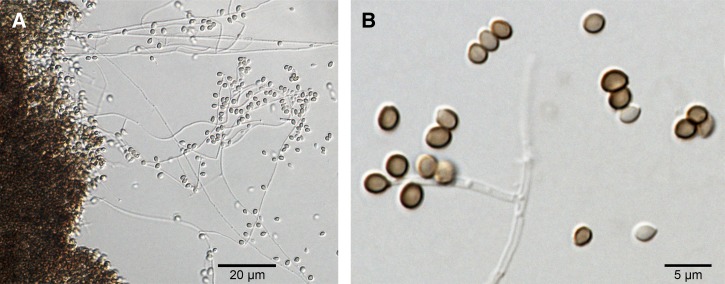
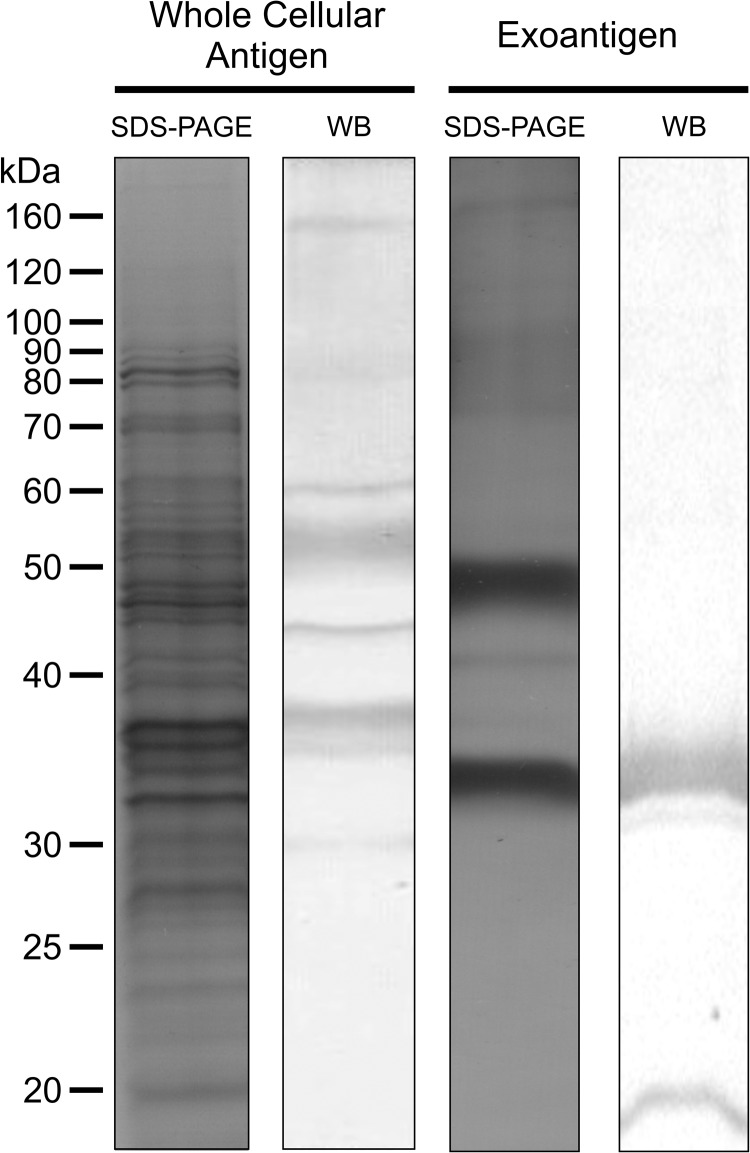
Sporotrichosis is a polymorphic disease of humans and animals, which is acquired via traumatic inoculation of Sporothrix propagules into cutaneous or subcutaneous tissue. The etiological agents are in a clinical complex, which includes Sporothrix brasiliensis, Sporothrix schenckii, Sporothrix globosa, and Sporothrix luriei, each of which has specific epidemiological and virulence characteristics. Classical manifestation in humans includes a fixed localized lesion at the site of trauma plus lymphocutaneous sporotrichosis with fungal spreading along the lymphatic channels. Atypical sporotrichosis is a challenge to diagnosis because it can mimic many other dermatological diseases. We report an unusual, itraconazole-resistant cutaneous lesion of sporotrichosis in a 66-year-old Brazilian man. Histopathological examination of the skin revealed vascular and fibroblastic proliferation with chronic granulomatous infiltrate composed of multinucleated giant cells. Sporothrix were isolated from the skin lesion, and phylogenetic analyses confirmed it to be sporotrichosis due to S. globosa, a widespread pathogen. Immunoblotting analysis showed several IgG-reactive molecules in autochthonous preparations of the whole cellular proteins (160, 80, 60, 55, 46, 38, 35, and 30 kDa) and exoantigen (35 and 33 kDa). The patient was first unsuccessfully treated with daily itraconazole, and then successfully treated with potassium iodide.
© The American Society of Tropical Medicine and Hygiene.
Figures


References
-
- Chakrabarti A, Bonifaz A, Gutierrez-Galhardo MC, Mochizuki T, Li S. Global epidemiology of sporotrichosis. Med Mycol. 2015;53:3–14. - PubMed
-
- Zhang Y, Hagen F, Stielow B, Rodrigues AM, Samerpitak K, Zhou X, Feng P, Yang L, Chen M, Deng S, Li S, Liao W, Li R, Li F, Meis JF, Guarro J, Teixeira M, Al-Zahrani HS, Camargo ZP, Zhang L, de Hoog GS. Phylogeography and evolutionary patterns in Sporothrix spanning more than 14000 human and animal case reports. Persoonia. 2015;35:1–20. - PMC - PubMed
-
- Bonifaz A, Vázquez-González D. Diagnosis and treatment of lymphocutaneous sporotrichosis: what are the options? Curr Fungal Infect Rep. 2013;7:252–259.
-
- Pappas PG, Tellez I, Deep AE, Nolasco D, Holgado W, Bustamante B. Sporotrichosis in Peru: description of an area of hyperendemicity. Clin Infect Dis. 2000;30:65–70. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
