Posterior Spinal Artery Aneurysm Presenting with Leukocytoclastic Vasculitis
- PMID: 27114966
- PMCID: PMC4842908
- DOI: 10.7461/jcen.2016.18.1.42
Posterior Spinal Artery Aneurysm Presenting with Leukocytoclastic Vasculitis
Abstract
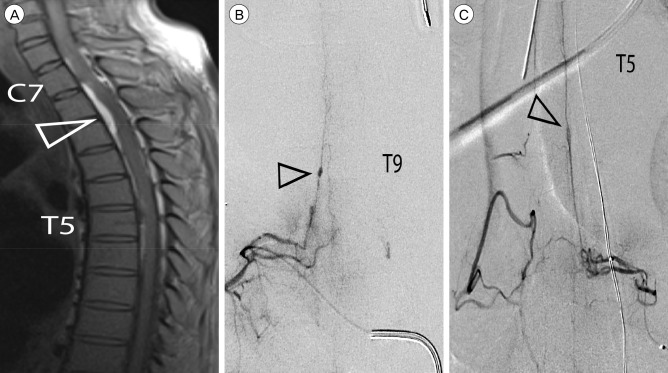
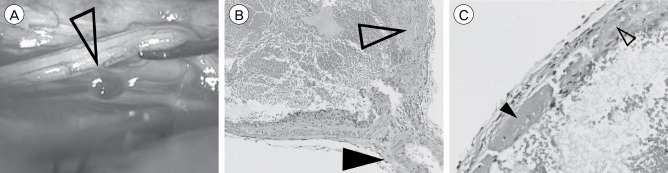
Rupture of isolated posterior spinal artery (PSA) aneurysms is a rare cause of subarachnoid hemorrhage (SAH) that presents unique diagnostic challenges owing to a nuanced clinical presentation. Here, we report on the diagnosis and management of the first known case of an isolated PSA aneurysm in the context of leukocytoclastic vasculitis. A 53-year-old male presented to an outside institution with acute bilateral lower extremity paralysis 9 days after admission for recurrent cellulitis. Early magnetic resonance imaging was read as negative and repeat imaging 15 days after presentation revealed SAH and a compressive spinal subdural hematoma. Angiography identified a PSA aneurysm at T9, as well as other areas suspicious for inflammatory or post-hemorrhagic reactive changes. The patient underwent a multilevel laminectomy for clot evacuation and aneurysm resection to prevent future hemorrhage and to establish a diagnosis. The postoperative course was complicated by medical issues and led to the diagnosis of leukocytoclastic vasculitis that may have predisposed the patient to aneurysm development. Literature review reveals greater mortality for cervical lesions than thoracolumbar lesions and that the presence of meningitic symptoms portents better functional outcome than symptoms of cord compression. The outcome obtained in this case is consistent with outcomes reported in the literature.
Keywords: Aneurysm; Hypersensitivity vasculitis; Leukocytoclastic vasculitis; Posterior spinal artery syndrome; Spinal cord vascular diseases; Subarachnoid hemorrhage.
Conflict of interest statement
Figures

Similar articles
-
Subarachnoid Hemorrhage due to Ruptured Spinal Artery Aneurysm: A Diagnostic Challenge.Case Rep Neurol. 2020 Dec 14;12(Suppl 1):169-175. doi: 10.1159/000507953. eCollection 2020 Sep-Dec. Case Rep Neurol. 2020. PMID: 33505290 Free PMC article.
-
Posterior spinal artery aneurysm as an unlikely culprit for perimesencephalic pattern subarachnoid hemorrhage: illustrative case.J Neurosurg Case Lessons. 2021 May 31;1(22):CASE21103. doi: 10.3171/CASE21103. eCollection 2021 May 31. J Neurosurg Case Lessons. 2021. PMID: 35855466 Free PMC article.
-
Isolated abducens nerve palsy associated with subarachnoid hemorrhage: a localizing sign of ruptured posterior inferior cerebellar artery aneurysms.J Neurosurg. 2018 Jun;128(6):1830-1838. doi: 10.3171/2017.2.JNS162951. Epub 2017 Sep 1. J Neurosurg. 2018. PMID: 28862551
-
A ruptured posterior communicating artery aneurysm presenting as tentorial and spinal isolated subdural hemorrhage: a case report and literature review.BMC Neurol. 2020 Mar 18;20(1):102. doi: 10.1186/s12883-020-01682-8. BMC Neurol. 2020. PMID: 32188416 Free PMC article. Review.
-
Spinal subarachnoid hemorrhage and aneurysms.Handb Clin Neurol. 2017;143:215-223. doi: 10.1016/B978-0-444-63640-9.00020-5. Handb Clin Neurol. 2017. PMID: 28552143 Review.
Cited by
-
An isolated ruptured spinal aneurysm presents with a thalamic Infarct: case report.BMC Neurol. 2021 Feb 3;21(1):52. doi: 10.1186/s12883-021-02055-5. BMC Neurol. 2021. PMID: 33535981 Free PMC article.
-
Ruptured isolated spinal artery aneurysms: Case series of five patients and a review of the literature on management strategies.Interv Neuroradiol. 2025 Jun;31(3):402-413. doi: 10.1177/15910199221149562. Epub 2023 Jan 10. Interv Neuroradiol. 2025. PMID: 36628492 Free PMC article. Review.
References
-
- Cavusoglu H, Ozdilmac A, Sahin Y, Aydin Y. Isolated posterior spinal artery aneurysm causing intracranial acute subarachnoidal hemorrhage. Acta Neurochir (Wien) 2010 Apr;152(4):721–724. - PubMed
-
- Doppman JL, Di Chiro G, Glancy DL. Collateral circulation through dilated spinal cord arteries in aortic coarctation and extraspinal arteriovenous shunts. An arteriographic study. Clin Radiol. 1969 Apr;20(2):192–197. - PubMed
-
- Fody EP, Netsky MG, Mrak RE. Subarachnoid spinal hemorrhage in a case of systemic lupus erythematosus. Arch Neurol. 1980 Mar;37(3):173–174. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous