

Diagnosis, Treatment, and Prevention of Lyme Disease, Human Granulocytic Anaplasmosis, and Babesiosis: A Review
- PMID: 27115378
- PMCID: PMC7758915
- DOI: 10.1001/jama.2016.2884
Diagnosis, Treatment, and Prevention of Lyme Disease, Human Granulocytic Anaplasmosis, and Babesiosis: A Review
Abstract
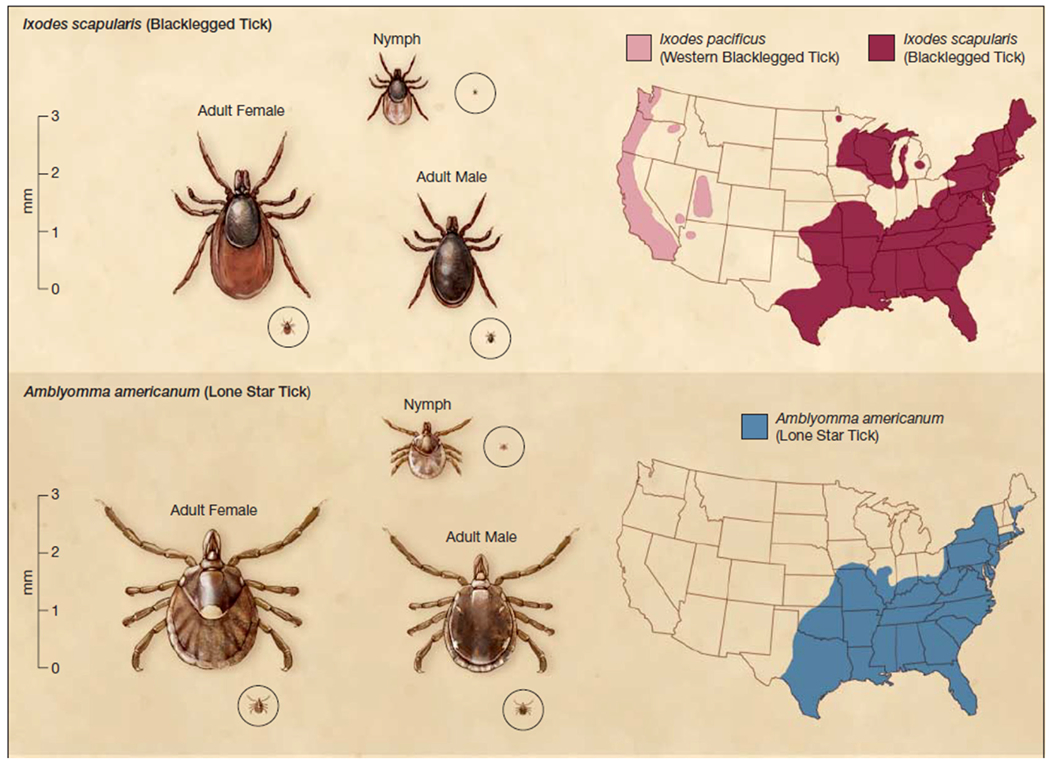
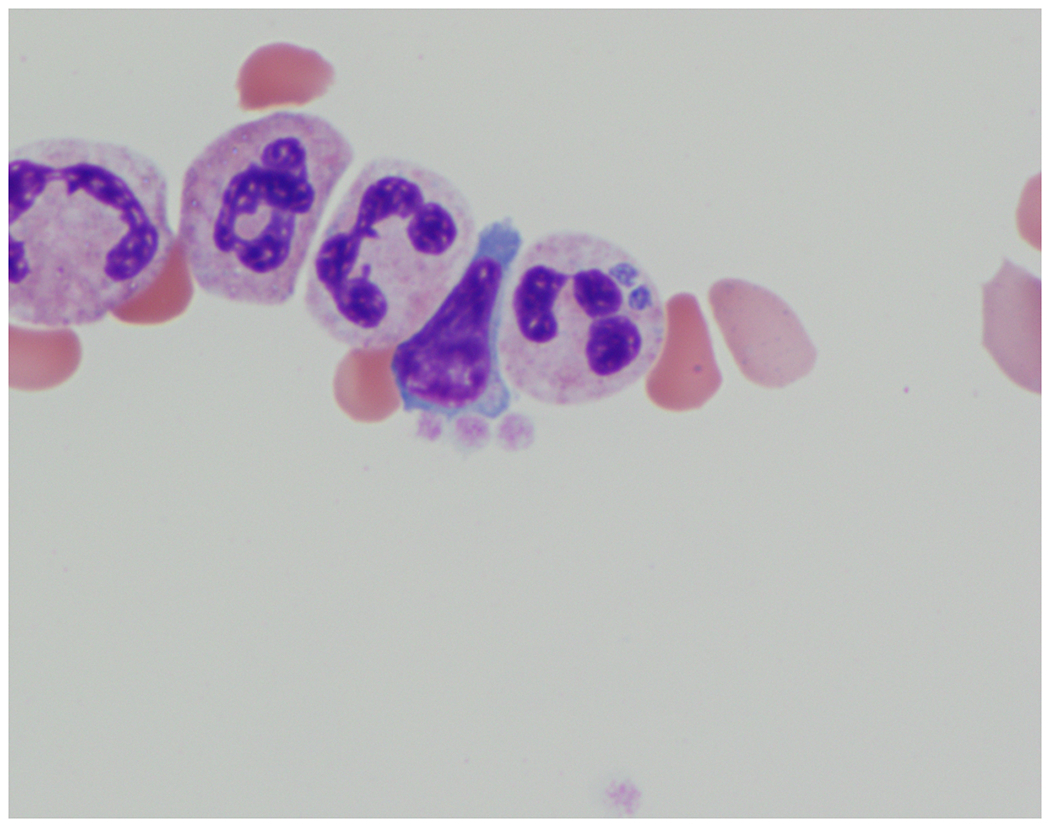
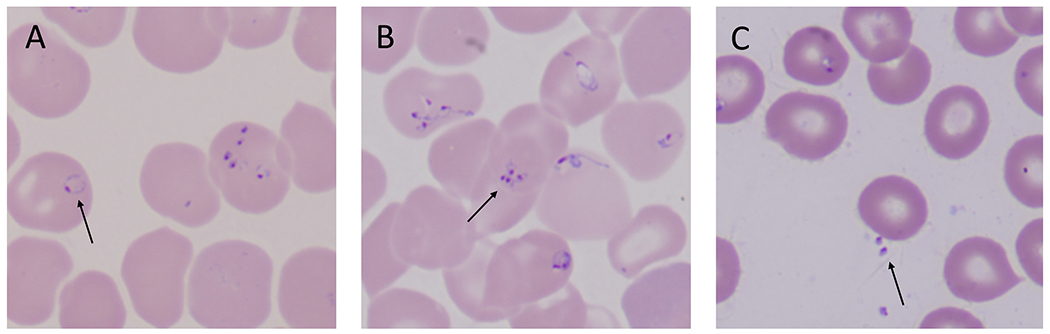
Importance: Lyme disease, human granulocytic anaplasmosis (HGA), and babesiosis are emerging tick-borne infections.
Objective: To provide an update on diagnosis, treatment, and prevention of tick-borne infections.
Evidence review: Search of PubMed and Scopus for articles on diagnosis, treatment, and prevention of tick-borne infections published in English from January 2005 through December 2015.
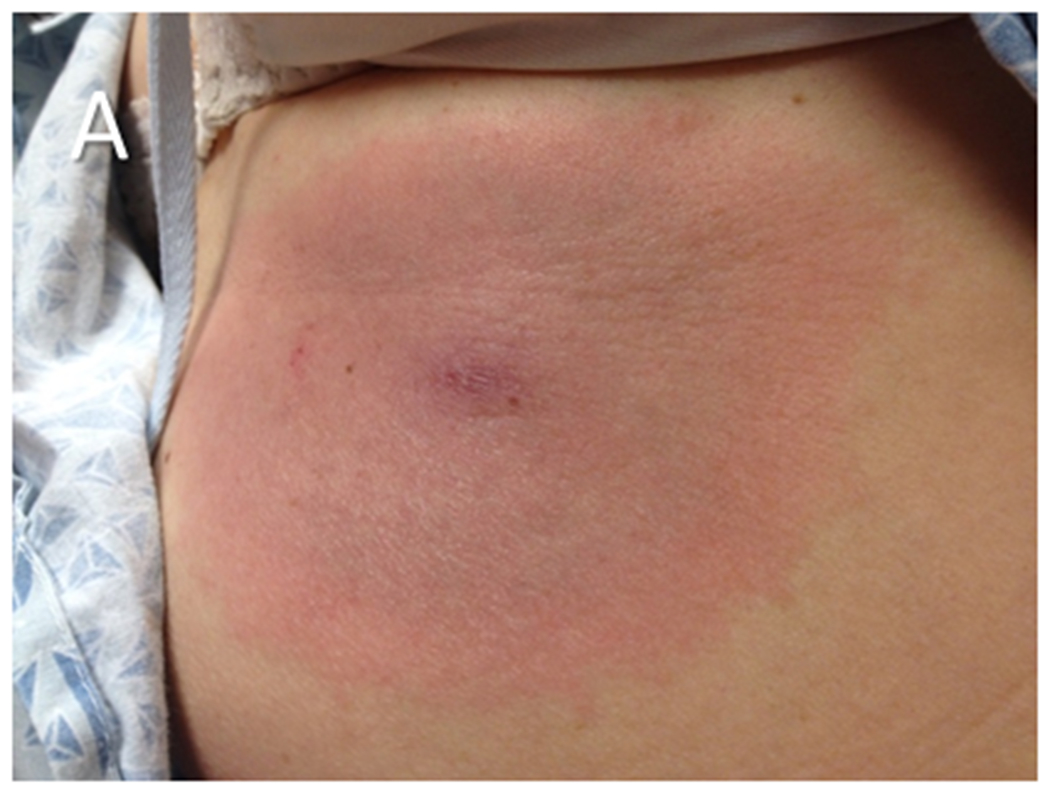
Findings: The search yielded 3550 articles for diagnosis and treatment and 752 articles for prevention. Of these articles, 361 were reviewed in depth. Evidence supports the use of US Food and Drug Administration-approved serologic tests, such as an enzyme immunoassay (EIA), followed by Western blot testing, to diagnose extracutaneous manifestations of Lyme disease. Microscopy and polymerase chain reaction assay of blood specimens are used to diagnose active HGA and babesiosis. The efficacy of oral doxycycline, amoxicillin, and cefuroxime axetil for treating Lyme disease has been established in multiple trials. Ceftriaxone is recommended when parenteral antibiotic therapy is recommended. Multiple trials have shown efficacy for a 10-day course of oral doxycycline for treatment of erythema migrans and for a 14-day course for treatment of early neurologic Lyme disease in ambulatory patients. Evidence indicates that a 10-day course of oral doxycycline is effective for HGA and that a 7- to 10-day course of azithromycin plus atovaquone is effective for mild babesiosis. Based on multiple case reports, a 7- to 10-day course of clindamycin plus quinine is often used to treat severe babesiosis. A recent study supports a minimum of 6 weeks of antibiotics for highly immunocompromised patients with babesiosis, with no parasites detected on blood smear for at least the final 2 weeks of treatment.
Conclusions and relevance: Evidence is evolving regarding the diagnosis, treatment, and prevention of Lyme disease, HGA, and babesiosis. Recent evidence supports treating patients with erythema migrans for no longer than 10 days when doxycycline is used and prescription of a 14-day course of oral doxycycline for early neurologic Lyme disease in ambulatory patients. The duration of antimicrobial therapy for babesiosis in severely immunocompromised patients should be extended to 6 weeks or longer.
Figures
References
-
- anonymous. Notifiable diseases and mortality tables. MMWR Morb Mortal Wkly Rep. 2016;64:ND-923–ND-940. - PubMed
-
- Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43(9):1089–1134. - PubMed
-
- Steere AC. Lyme disease. N Engl J Med. 2001;345(2):115–125. - PubMed
-
- Halperin JJ. Nervous system Lyme disease. Infect Dis Clin North Am. 2015;29(2):241–253. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
