

Mucus Hyperconcentration as a Unifying Aspect of the Chronic Bronchitic Phenotype
- PMID: 27115951
- PMCID: PMC5015722
- DOI: 10.1513/AnnalsATS.201507-455KV
Mucus Hyperconcentration as a Unifying Aspect of the Chronic Bronchitic Phenotype
Abstract
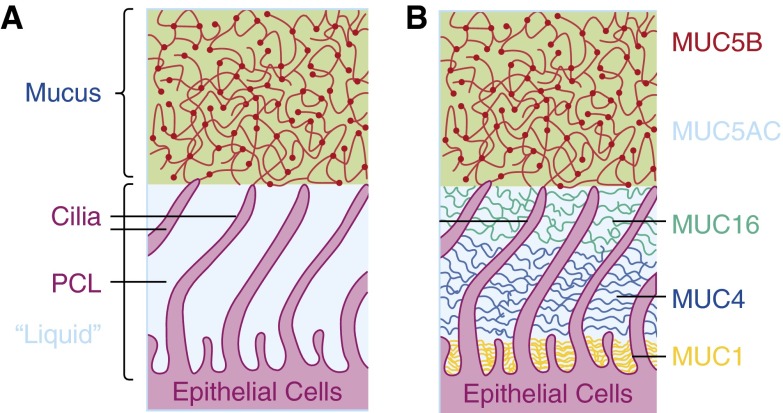
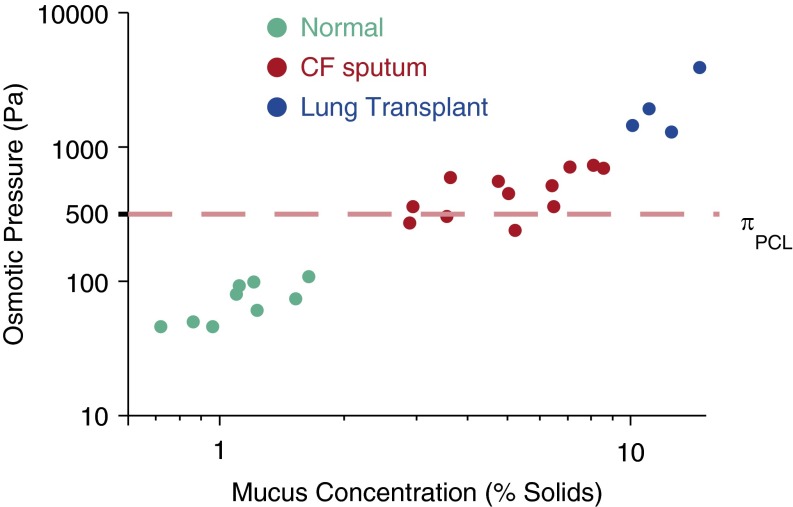
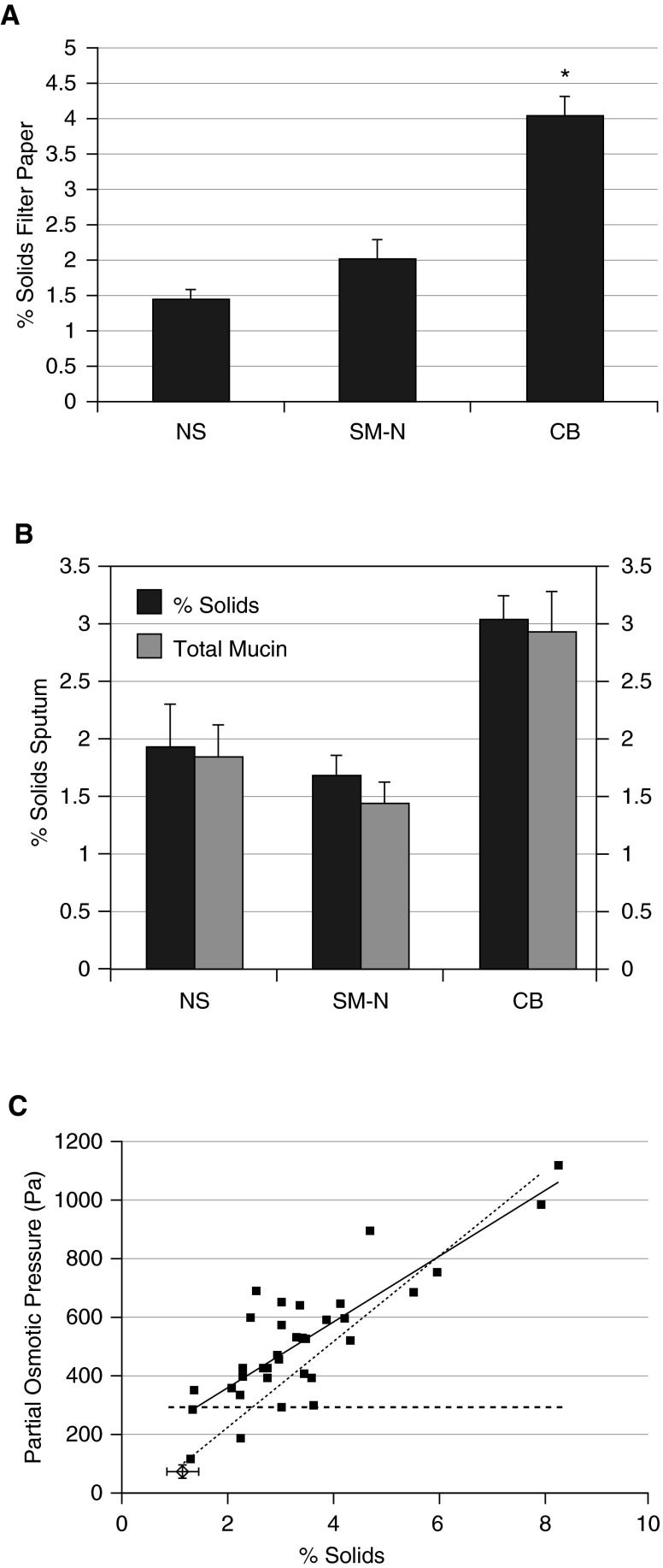
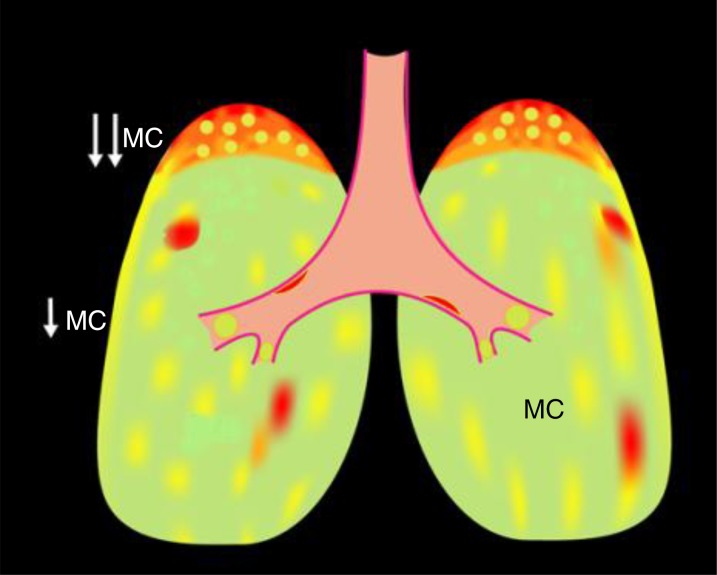
Abnormalities in mucus production and qualitative properties such as mucus hydration are central to the pathophysiology of airway disease including cystic fibrosis, asthma, and chronic bronchitis. In vitro air-liquid interface epithelial cell cultures demonstrate direct relationships between mucociliary transport, periciliary liquid (PCL) height, and mucus concentration (expressed as percent solids or partial osmotic pressure). In health, the osmotic modulus/pressure of the PCL exceeds that of the mucus layer, resulting in efficient, low-friction movement of mucus. In disease, through multiple mechanisms, the osmotic pressure of the mucus begins to exceed basal PCL values, resulting in compression of the cilia and slowing of mucus transport. The in vivo data in both cystic fibrosis and chronic bronchitis parallel in vitro data demonstrating that when mucus osmotic pressure is increased, mucociliary clearance is decreased. In chronic bronchitis, there is a direct correlation between FEV1 and percent solids of mucus, demonstrating a strong relationship between disease progression and mucus abnormalities. Animal models, based mechanistically on raised sodium absorption (and therefore water absorption) from airway surfaces, mimic the pathophysiology of chronic obstructive pulmonary disease. Collectively, these data suggest the importance of mucus concentration in the pathogenesis of airway disease. It is important to understand the precise mechanisms that result in mucus hyperconcentration, for example, mucin overproduction versus abnormal regulation of ion/water transport, which may be unique to and characteristic of each disease phenotype. The measurement of mucus concentration may be a simple method to diagnose chronic bronchitis, monitor its progression, and serve as a biomarker for development of new therapies.
Keywords: chronic bronchitis; mucociliary clearance; mucus; osmotic pressure.
Figures
References
-
- Wanner A, Salathé M, O’Riordan TG. Mucociliary clearance in the airways. Am J Respir Crit Care Med. 1996;154:1868–1902. - PubMed
-
- Munkholm M, Mortensen J. Mucociliary clearance: pathophysiological aspects. Clin Physiol Funct Imaging. 2014;34:171–177. - PubMed
-
- Rubinstein M, Colby RH. Polymer physics. Oxford: Oxford University Press; 2003.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
