

Hybrid intravascular imaging: recent advances, technical considerations, and current applications in the study of plaque pathophysiology
- PMID: 27118197
- PMCID: PMC5837589
- DOI: 10.1093/eurheartj/ehw097
Hybrid intravascular imaging: recent advances, technical considerations, and current applications in the study of plaque pathophysiology
Abstract
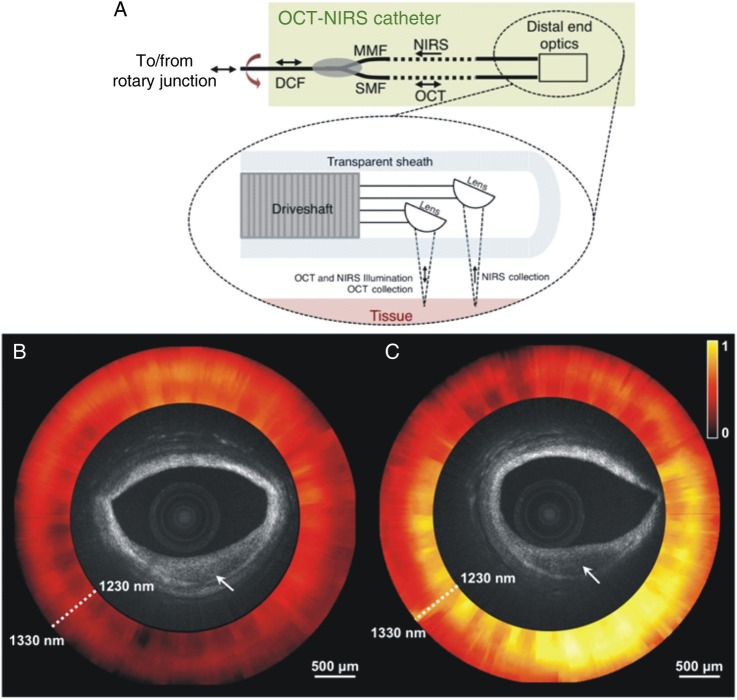
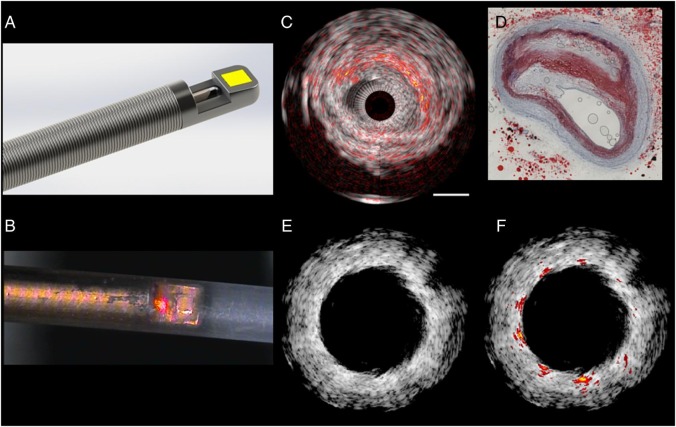
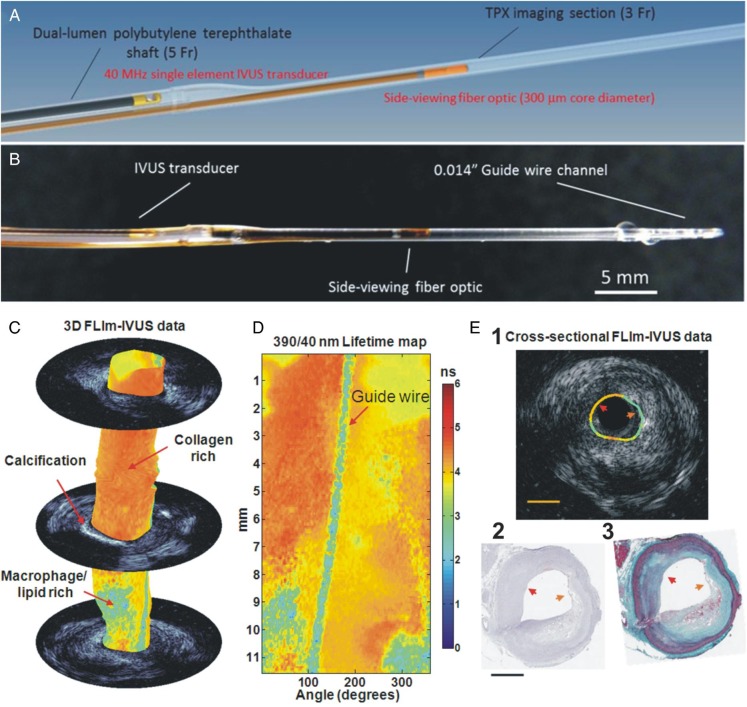
Cumulative evidence from histology-based studies demonstrate that the currently available intravascular imaging techniques have fundamental limitations that do not allow complete and detailed evaluation of plaque morphology and pathobiology, limiting the ability to accurately identify high-risk plaques. To overcome these drawbacks, new efforts are developing for data fusion methodologies and the design of hybrid, dual-probe catheters to enable accurate assessment of plaque characteristics, and reliable identification of high-risk lesions. Today several dual-probe catheters have been introduced including combined near infrared spectroscopy-intravascular ultrasound (NIRS-IVUS), that is already commercially available, IVUS-optical coherence tomography (OCT), the OCT-NIRS, the OCT-near infrared fluorescence (NIRF) molecular imaging, IVUS-NIRF, IVUS intravascular photoacoustic imaging and combined fluorescence lifetime-IVUS imaging. These multimodal approaches appear able to overcome limitations of standalone imaging and provide comprehensive visualization of plaque composition and plaque biology. The aim of this review article is to summarize the advances in hybrid intravascular imaging, discuss the technical challenges that should be addressed in order to have a use in the clinical arena, and present the evidence from their first applications aiming to highlight their potential value in the study of atherosclerosis.
Keywords: Coronary atherosclerosis; Hybrid imaging; Intravascular imaging.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2016. For permissions please email: journals.permissions@oup.com.
Figures
References
-
- Potkin BN, Bartorelli AL, Gessert JM, Neville RF, Almagor Y, Roberts WC, Leon MB. Coronary artery imaging with intravascular high-frequency ultrasound. Circulation 1990;81:1575–1585. - PubMed
-
- Sano K, Kawasaki M, Ishihara Y, Okubo M, Tsuchiya K, Nishigaki K, Zhou X, Minatoguchi S, Fujita H, Fujiwara H. Assessment of vulnerable plaques causing acute coronary syndrome using integrated backscatter intravascular ultrasound. J Am Coll Cardiol 2006;47:734–741. - PubMed
-
- Uemura S, Ishigami K, Soeda T, Okayama S, Sung JH, Nakagawa H, Somekawa S, Takeda Y, Kawata H, Horii M, Saito Y. Thin-cap fibroatheroma and microchannel findings in optical coherence tomography correlate with subsequent progression of coronary atheromatous plaques. Eur Heart J 2012;33:78–85. - PubMed
-
- Pu J, Mintz GS, Biro S, Lee JB, Sum ST, Madden SP, Burke AP, Zhang P, He B, Goldstein JA, Stone GW, Muller JE, Virmani R, Maehara A. Insights into echo-attenuated plaques, echolucent plaques, and plaques with spotty calcification: novel findings from comparisons among intravascular ultrasound, near-infrared spectroscopy, and pathological histology in 2,294 human coronary artery segments. J Am Coll Cardiol 2014;63:2220–2233. - PubMed
-
- Manfrini O, Mont E, Leone O, Arbustini E, Eusebi V, Virmani R, Bugiardini R. Sources of error and interpretation of plaque morphology by optical coherence tomography. Am J Cardiol 2006;98:156–159. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
