

Mass drug administration: the importance of synchrony
- PMID: 27118395
- PMCID: PMC6201266
- DOI: 10.1093/imammb/dqw005
Mass drug administration: the importance of synchrony
Abstract
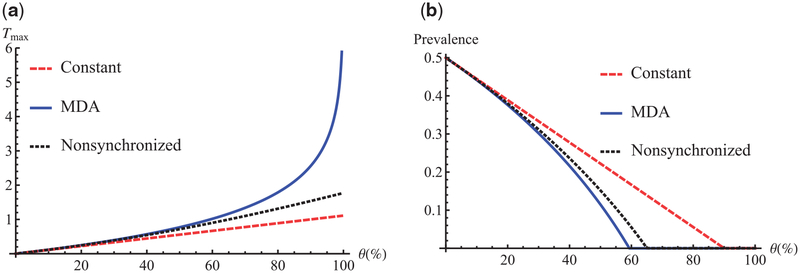
Mass drug administration, a strategy in which all individuals in a population are subject to treatment without individual diagnosis, has been recommended by the World Health Organization for controlling and eliminating several neglected tropical diseases, including trachoma and soil-transmitted helminths. In this article, we derive effective reproduction numbers and average post-treatment disease prevalences of a simple susceptible-infectious-susceptible epidemic model with constant, impulsive synchronized and non-synchronized drug administration strategies. In the non-synchronized model, the individuals in the population are treated at most once per period and their treatment times are uniformly distributed. Mathematically, the set of pulses for the non-synchronized model has the cardinality of the continuum. We show that synchronized and constant strategies are, respectively, the most and least effective treatments in disease control. Elimination through synchronized treatment is always possible when adequate drug efficacy and coverage are fulfilled and sustained. For a strategy with multiple rounds of synchronized treatment per period, the average post-treatment prevalence is irrelevant what the time differences between treatments are, as long as there are the same number of treatments per period.
Keywords: cost-effectiveness; effective reproduction number; non-synchronized treatment; synchronized treatment; trachoma.
© The authors 2016. Published by Oxford University Press on behalf of the Institute of Mathematics and its Applications. All rights reserved.
Figures



References
-
- Anderson R, Hollingsworth TD, Truscott J & Brooker S (2012) Optimisation of mass chemotherapy to control soil-transmitted helminth infection. Lancet, 379, 289–290. - PubMed
-
- Bacaër N & Ouifki R (2007) Growth rate and basic reproduction number for population models with a simple periodic factor. Math. Biosci, 210, 647–658. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
