

Smoking and Adverse Outcomes in Patients With CKD: The Study of Heart and Renal Protection (SHARP)
- PMID: 27118687
- PMCID: PMC4996629
- DOI: 10.1053/j.ajkd.2016.02.052
Smoking and Adverse Outcomes in Patients With CKD: The Study of Heart and Renal Protection (SHARP)
Abstract
Background: The absolute and relative importance of smoking to vascular and nonvascular outcomes in people with chronic kidney disease (CKD), as well its relevance to kidney disease progression, is uncertain.
Study design: Observational study.
Setting & participants: 9,270 participants with CKD enrolled in SHARP.
Predictor: Baseline smoking status (current, former, and never).
Outcomes: Vascular events, site-specific cancer, ESRD, rate of change in estimated glomerular filtration rate (eGFR), and cause-specific mortality.
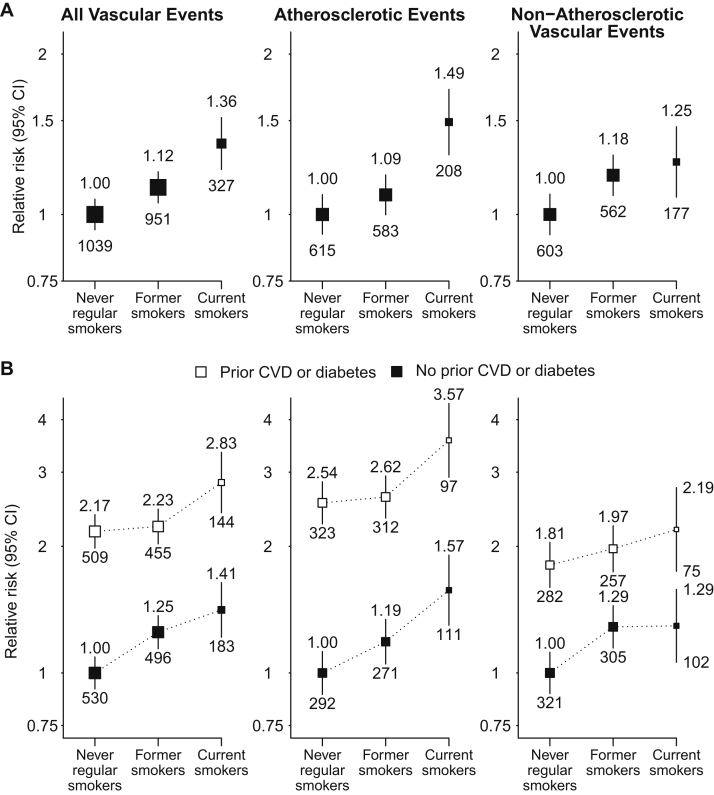
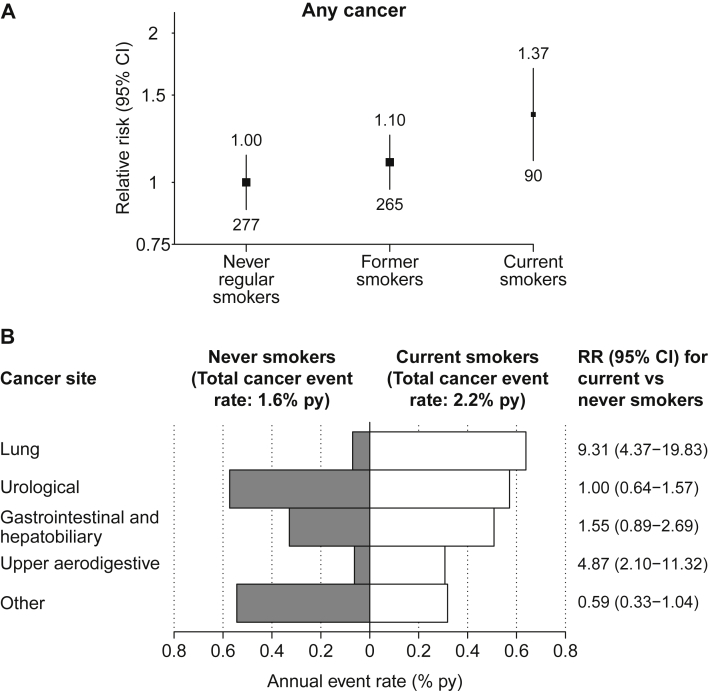
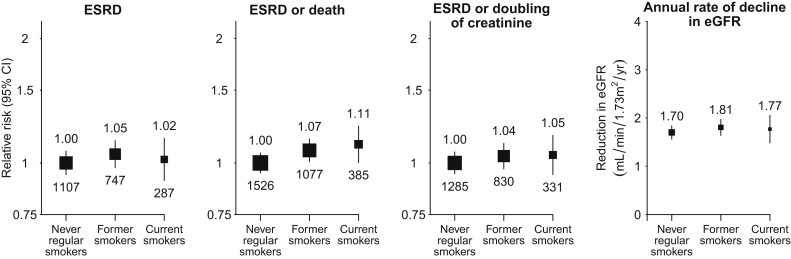
Results: At baseline, 1,243 (13%) participants were current smokers (median consumption, 10 cigarettes/day); 3,272 (35%), former smokers; and 4,755 (51%), never smokers. Median follow-up was 4.9 years. Vascular event rates were 36% higher for current than never smokers (2,317 events; relative risk [RR], 1.36; 95% CI, 1.19-1.55), reflecting increases in both atherosclerotic (RR, 1.49; 95% CI, 1.26-1.76) and nonatherosclerotic (RR, 1.25; 95% CI, 1.05-1.50) events. Cancer was 37% higher among current smokers (632 events; RR, 1.37; 95% CI, 1.07-1.76), with the biggest RRs for lung (RR, 9.31; 95% CI, 4.37-19.83) and upper aerodigestive tract (RR, 4.87; 95% CI, 2.10-11.32) cancers. For 6,245 patients not receiving dialysis at baseline, ESRD incidence did not differ significantly between current and never smokers (2,141 events; RR, 1.02; 95% CI, 0.89-1.17), nor did estimated rate of change in eGFR (current smokers, -1.77±0.14 [SE]; never smokers, -1.70±0.07mL/min/1.73m(2) per year). All-cause mortality was 48% higher among current smokers (2,257 events; RR, 1.48; 95% CI, 1.30-1.70), with significant increases in vascular (RR, 1.35; 95% CI, 1.07-1.69) and nonvascular (RR, 1.60; 95% CI, 1.34-1.91) causes of death, especially cancer (RR, 2.32; 95% CI, 1.58-3.40) and respiratory (RR, 2.25; 95% CI, 1.51-3.35) mortality.
Limitations: Smoking status not assessed during follow-up.
Conclusions: In this study of patients with CKD, smoking significantly increased the risks for vascular and nonvascular morbidity and mortality, but was not associated with kidney disease progression. The associations with vascular and neoplastic disease are in keeping with those observed in the general population and are likely modifiable by cessation.
Keywords: Cigarette smoking; Study of Heart and Renal Protection (SHARP); cancer; cause-specific mortality; chronic kidney disease (CKD); disease progression; end-stage renal disease (ESRD); estimated glomerular filtration rate (eGFR); risk factor; tobacco; vascular events; vascular morbidity.
Copyright © 2016 The Authors. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Smoking, Vascular Events, and ESRD in Patients With CKD.Am J Kidney Dis. 2016 Sep;68(3):338-40. doi: 10.1053/j.ajkd.2016.06.004. Am J Kidney Dis. 2016. PMID: 27561666 Free PMC article. No abstract available.
References
-
- Carter B.D., Abnet C.C., Feskanich D. Smoking and mortality–beyond established causes. N Engl J Med. 2015;372(7):631–640. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
