

Gastrointestinal Complications After Bariatric Surgery
- PMID: 27118949
- PMCID: PMC4843041
Gastrointestinal Complications After Bariatric Surgery
Abstract
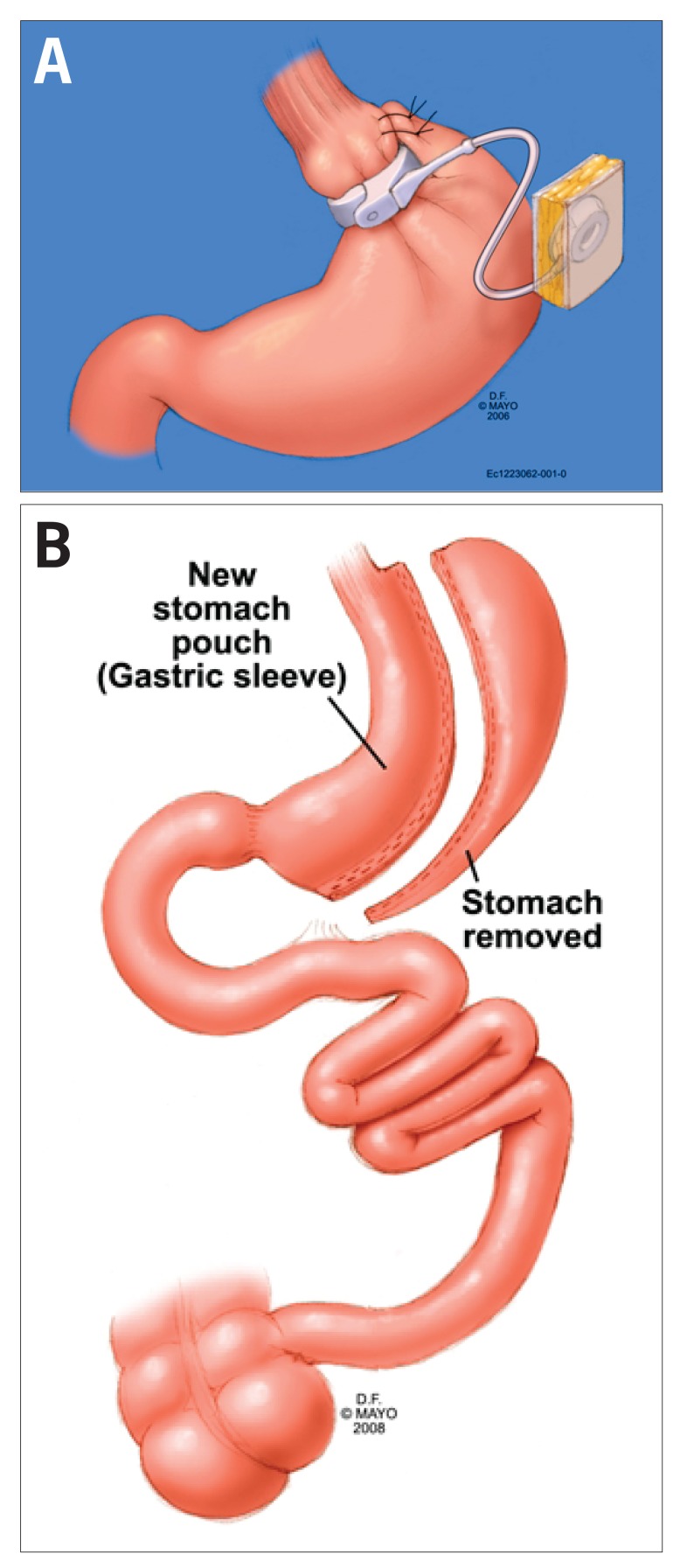
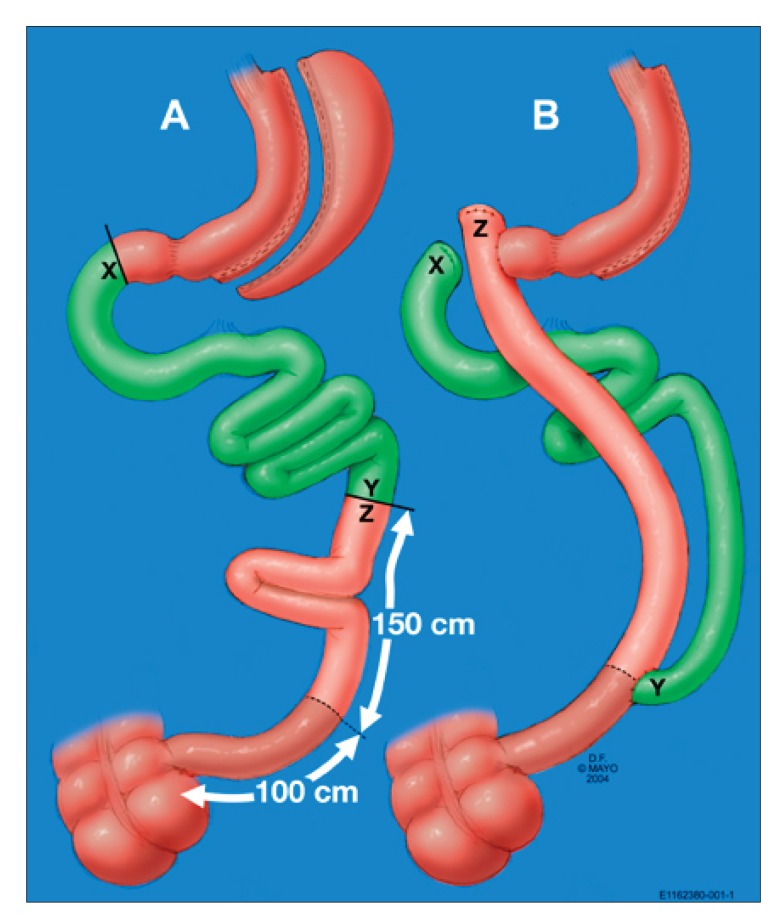
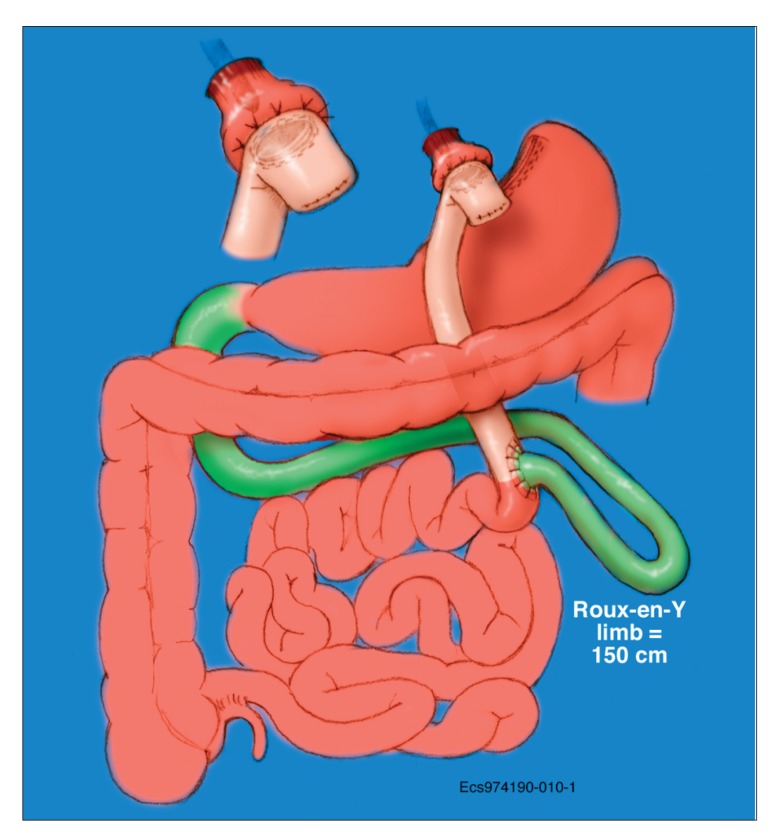
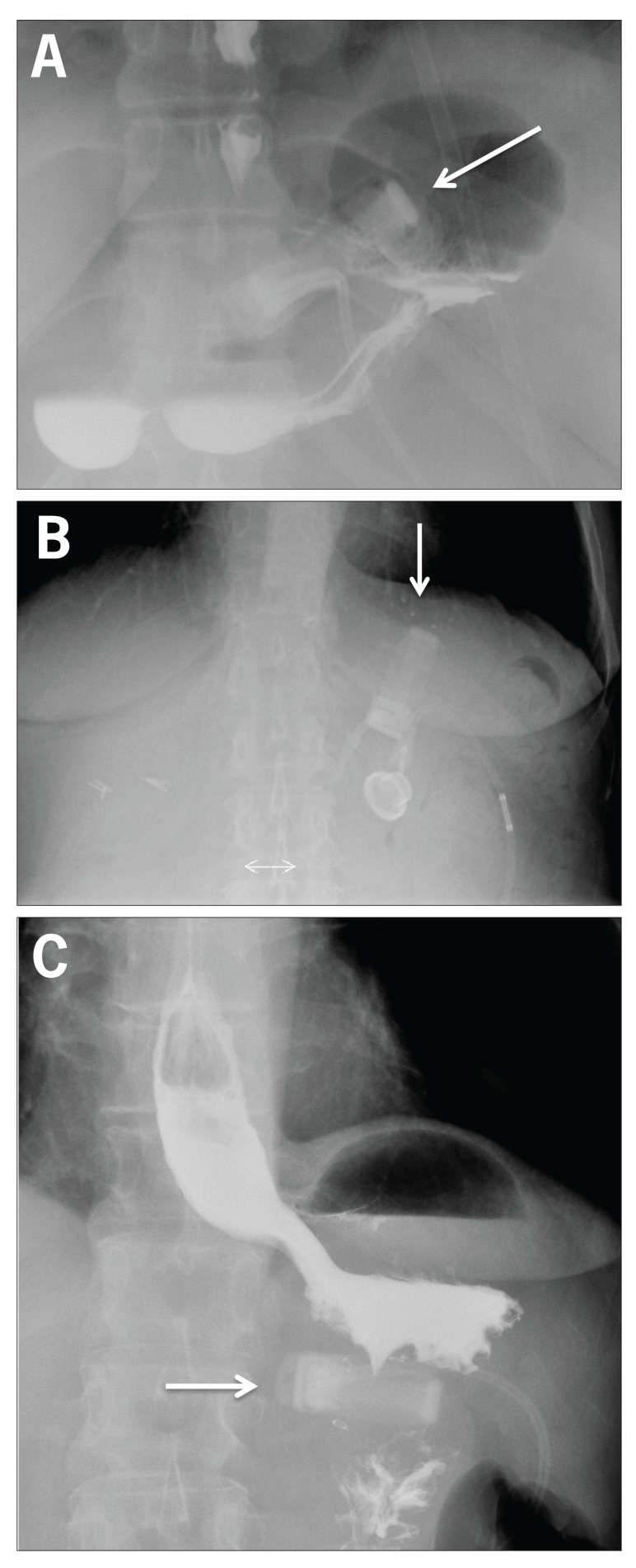
Bariatric surgery is increasingly being performed in the medically complicated obese population as convincing data continue to mount, documenting the success of surgery not only in achieving meaningful weight loss but also in correcting obesity-related illnesses. Several surgical procedures with varying degrees of success and complications are currently being performed. This article discusses the short- and long-term gastrointestinal complications for the 4 most common bariatric surgical procedures: laparoscopic adjustable gastric banding, vertical sleeve gastrectomy, Roux-en-Y gastric bypass, and biliopancreatic diversion with duodenal switch.
Keywords: Bariatric surgery; biliopancreatic diversion; duodenal switch; gastric bypass; gastrointestinal complications; vertical sleeve gastrectomy.
Figures
References
-
- Gastrointestinal surgery for severe obesity: National Institutes of Health Consensus Development Conference Statement. Am J Clin Nutr. 1992;55(2 suppl):615S–619S. - PubMed
-
- Flegal KM. Epidemiologic aspects of overweight and obesity in the United States. Physiol Behav. 2005;86(5):599–602. - PubMed
-
- Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010. JAMA. 2012;307(5):491–497. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials