

Institutional Delivery and Satisfaction among Indigenous and Poor Women in Guatemala, Mexico, and Panama
- PMID: 27120070
- PMCID: PMC4847770
- DOI: 10.1371/journal.pone.0154388
Institutional Delivery and Satisfaction among Indigenous and Poor Women in Guatemala, Mexico, and Panama
Abstract
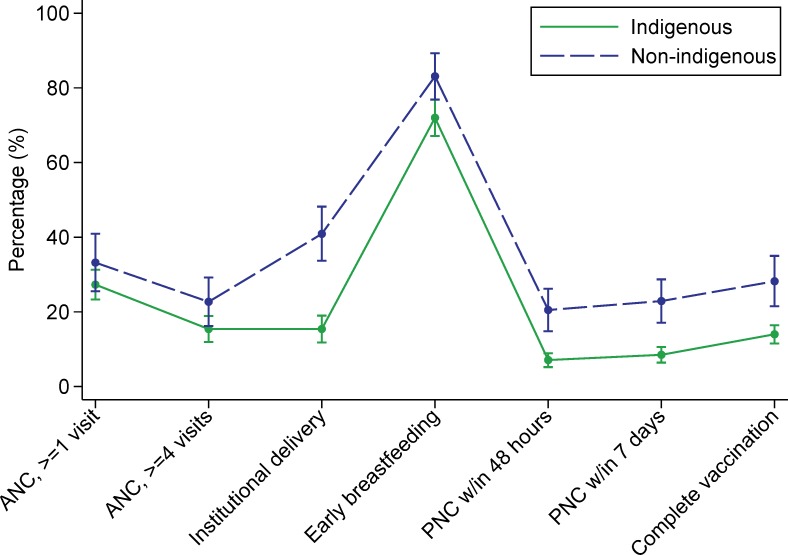
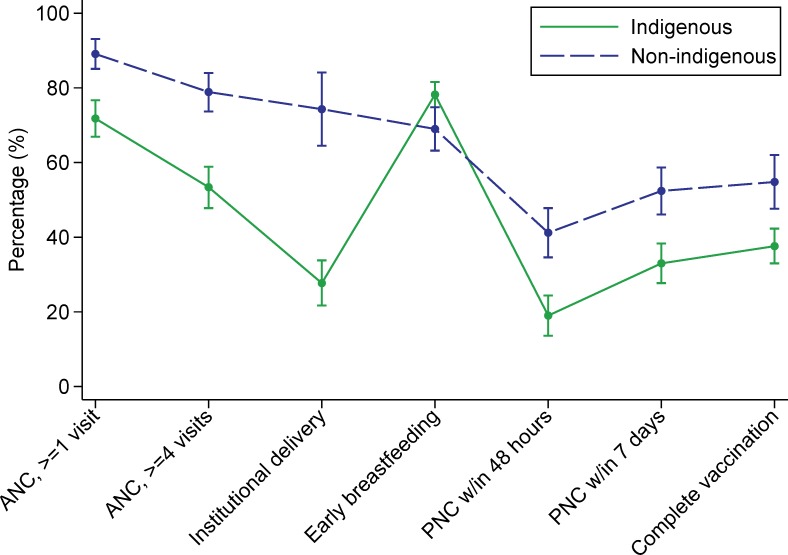
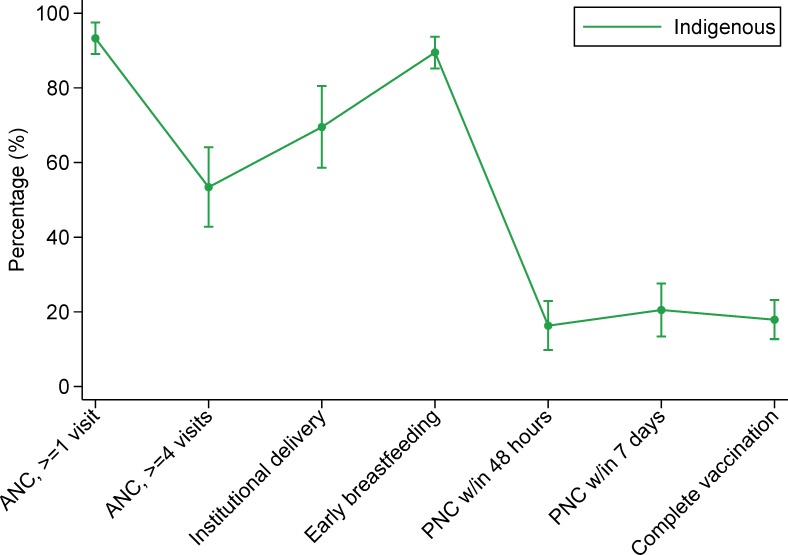
Indigenous women in Mesoamerica experience disproportionately high maternal mortality rates and are less likely to have institutional deliveries. Identifying correlates of institutional delivery, and satisfaction with institutional deliveries, may help improve facility utilization and health outcomes in this population. We used baseline surveys from the Salud Mesoamérica Initiative to analyze data from 10,895 indigenous and non-indigenous women in Guatemala and Mexico (Chiapas State) and indigenous women in Panama. We created multivariable Poisson regression models for indigenous (Guatemala, Mexico, Panama) and non-indigenous (Guatemala, Mexico) women to identify correlates of institutional delivery and satisfaction. Compared to their non-indigenous peers, indigenous women were substantially less likely to have an institutional delivery (15.2% vs. 41.5% in Guatemala (P<0.001), 29.1% vs. 73.9% in Mexico (P<0.001), and 70.3% among indigenous Panamanian women). Indigenous women who had at least one antenatal care visit were more than 90% more likely to have an institutional delivery (adjusted risk ratio (aRR) = 1.94, 95% confidence interval (CI): 1.44-2.61), compared to those who had no visits. Indigenous women who were advised to give birth in a health facility (aRR = 1.46, 95% CI: 1.18-1.81), primiparous (aRR = 1.44, 95% CI: 1.24-1.68), informed that she should have a Caesarean section (aRR = 1.41, 95% CI: 1.21-1.63), and had a secondary or higher level of education (aRR = 1.36, 95% CI: 1.04-1.79) also had substantially higher likelihoods of institutional delivery. Satisfaction among indigenous women was associated with being able to be accompanied by a community health worker (aRR = 1.15, 95% CI: 1.05-1.26) and facility staff speaking an indigenous language (aRR = 1.10, 95% CI: 1.02-1.19). Additional effort should be exerted to increase utilization of birthing facilities by indigenous and poor women in the region. Improving access to antenatal care and opportunities for higher-level education may increase institutional delivery rates, and providing culturally adapted services may improve satisfaction.
Conflict of interest statement
Figures
References
-
- Kassebaum NJ, Bertozzi-Villa A, Coggeshall MS, Shackelford KA, Steiner C, Heuton KR, et al. Global, regional, and national levels and causes of maternal mortality during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet. 2014;384: 980–1004. 10.1016/S0140-6736(14)60696-6 - DOI - PMC - PubMed
-
- Freyermuth-Enciso G, Cárdenas-Elizalde R. Evaluación del subregistro de la mortalidad materna en Los Altos de Chiapas mediante las estrategias RAMOS y RAMOS modificada. Salud Pública México. 2009;51: 450–457. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
