

Case Reports
doi: 10.1136/bcr-2016-215227.
Unusual case of intracranial dural AV fistula presenting with acute myelopathy
Affiliations
- PMID: 27122105
- PMCID: PMC4854136
- DOI: 10.1136/bcr-2016-215227
Item in Clipboard
Case Reports
Unusual case of intracranial dural AV fistula presenting with acute myelopathy
BMJ Case Rep.
.
Abstract
We present a case of intracranial arteriovenous fistula with perimedullary venous drainage presenting with acute myelopathy, which is an unusual presentation of this uncommon condition. Subsequent catheter angiogram defined the arterial feeders from the meningohypophyseal trunk and petrosal branch of the middle meningeal artery. The patient was successfully embolised, resulting in complete obliteration of the fistula, and significant resolution of brainstem and cervical cord changes along with clinical improvement.
2016 BMJ Publishing Group Ltd.
Figures
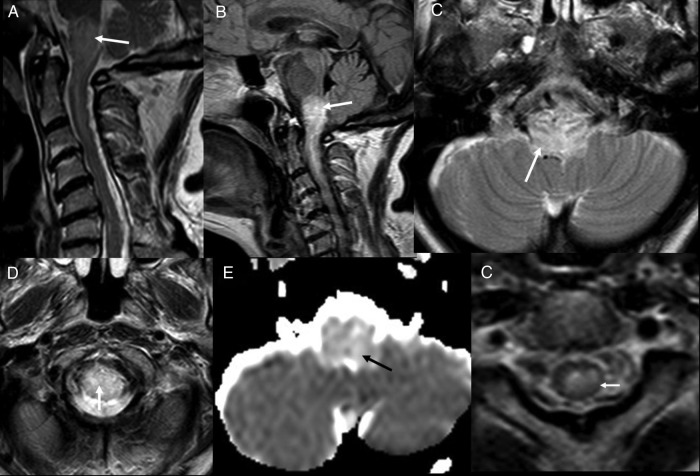
Initial MRI. T2 sagittal (A), FLAIR sagittal (B) and T2 axials (C and D) show presence of oedema in medulla and upper cervical cord (white arrow). ADC map (E) shows high ADC value suggestive of vasogenic oedema (black arrow). T2 axial (F) though upper cervical cord showing low peripheral T2 signal (white arrow). FLAIR, fluid attentuated inversion recovery; ADC, apparent diffusion coefficient.
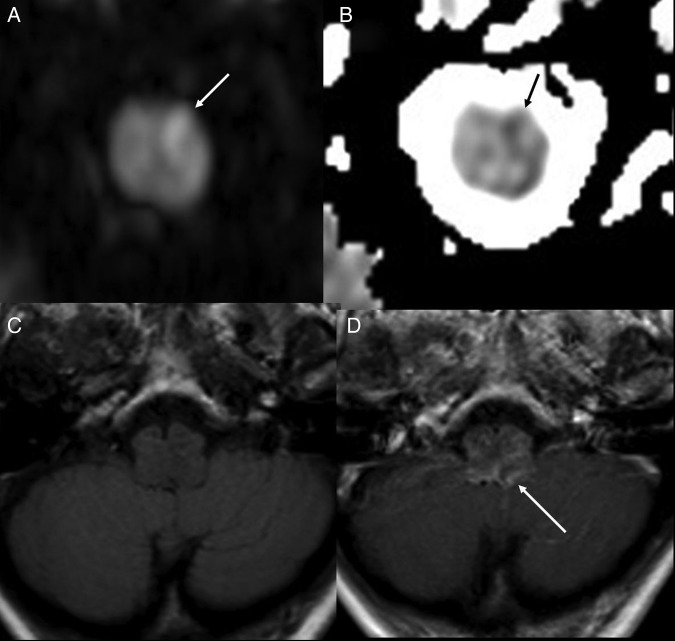
DWI (A) and ADC map (B), showing a probable small area of restricted diffusion (arrows) suggesting small recent infarct. T1 axial (C) and T1 axial post contrast (D) showing vascular congestion and enhancement (white arrow). DWI, diffusion weighted images; ICA, internal carotid artery.
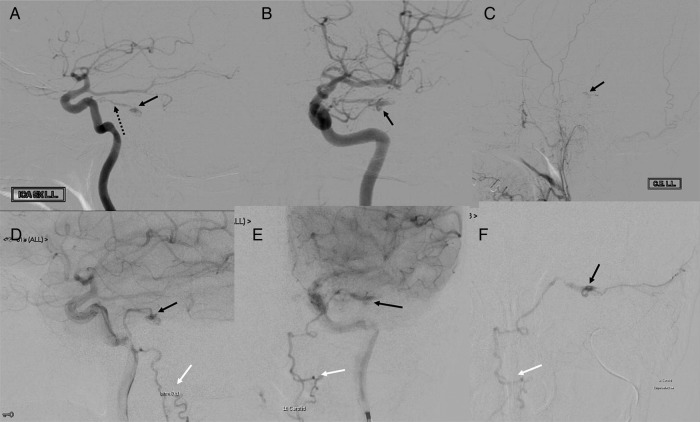
DSA. Left ICA injection. Lateral views (A and D) and AP views (B and E) showing MHT (broken arrow in A), site of fistula/nidus (black arrows) and perimedullary venous drainage (white arrows). Left ECA injection, lateral view (C), showing nidus (black arrow). Superselective MMA injection (F) showing site of fistula/nidus (black arrow) and perimedullary venous drainage (white arrow). AP, anteroposterior; DSA, digital subtraction angiography; ECA, external carotid artery; MHT, meningohypophyseal trunk; MMA, middle meningeal artery.
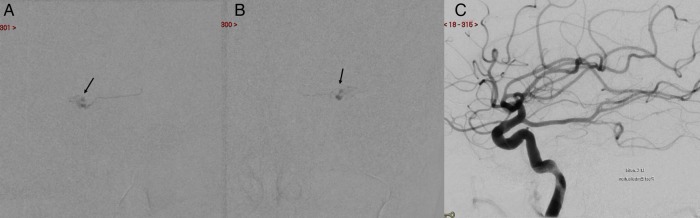
Embolisation. PHIL cast seen (black arrows in A and B). Postembolisation left ICA injection, lateral view (C), shows absence of fistula. PHIL, precipitating hydrophobic injectable liquid.
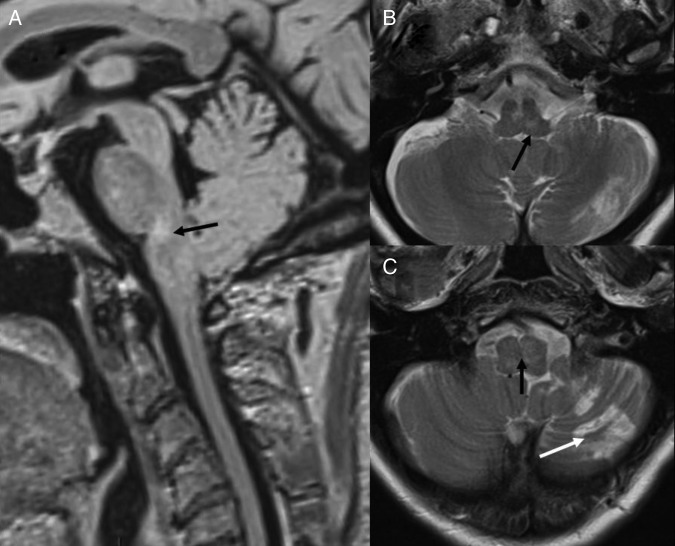
Follow-up MRI. FLAIR sagittal (A) and T2 axials (B and C) show significant resolution of oedema with some residual changes (black arrow) and left cerebellar infarct (white arrow in C).
References
-
- Ricolfi F, Manelfe C, Meder JF et al. . Intracranial dural arteriovenous fistulae with perimedullary venous drainage. Anatomical, clinical and therapeutic considerations. Neuroradiology 1999;41:803–12. - PubMed
-
- Chung SJ, Kim JS, Kim JC et al. . Intracranial dural arteriovenous fistulas: analysis of 60 patients. Cerebrovasc Dis 2002;13:79–88. - PubMed
-
- Newton TH, Cronqvist S. Involvement of dural arteries in intracranial arteriovenous malformations. Radiology 1969;93:1071–8. - PubMed
-
- Mahagne MH, Rogopoulos A, Paquis PH et al. . Fistules artérioveineuses durales intracraniennes a drainage veineux médullaire. Rev Neurol 1992;148:789–92. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical