

Inequalities in use of total hip arthroplasty for hip fracture: population based study
- PMID: 27122469
- PMCID: PMC4849171
- DOI: 10.1136/bmj.i2021
Inequalities in use of total hip arthroplasty for hip fracture: population based study
Abstract
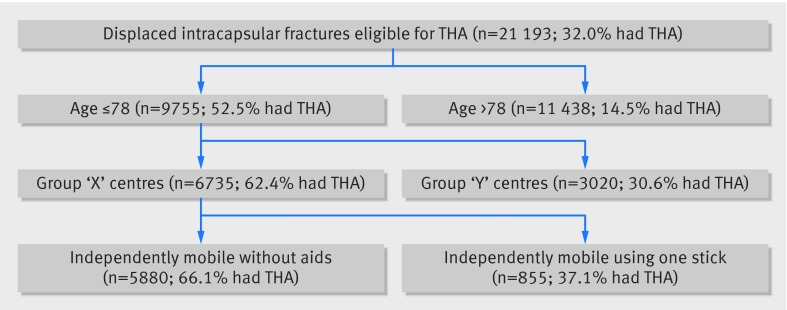
Objectives: To determine whether the use of total hip arthroplasty (THA) among individuals with a displaced intracapsular fracture of the femoral neck is based on national guidelines or if there are systematic inequalities.
Design: Observational cohort study using the National Hip Fracture Database (NHFD).
Setting: All hospitals that treat adults with hip fractures in England, Wales, and Northern Ireland.
Participants: Patients within the national database (all aged ≥60) who received operative treatment for a non-pathological displaced intracapsular hip fracture from 1 July 2011 to 31 April 2015.
Main outcome measures: Provision of THA to patients considered eligible under criteria published by the National Institute for Health and Care Excellence (NICE).
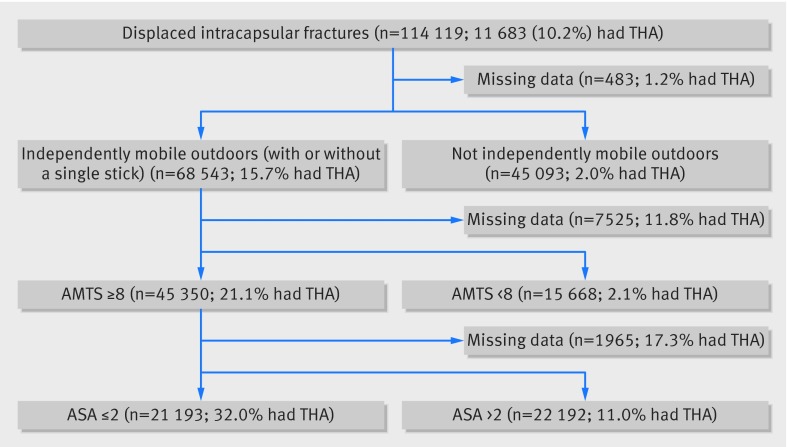
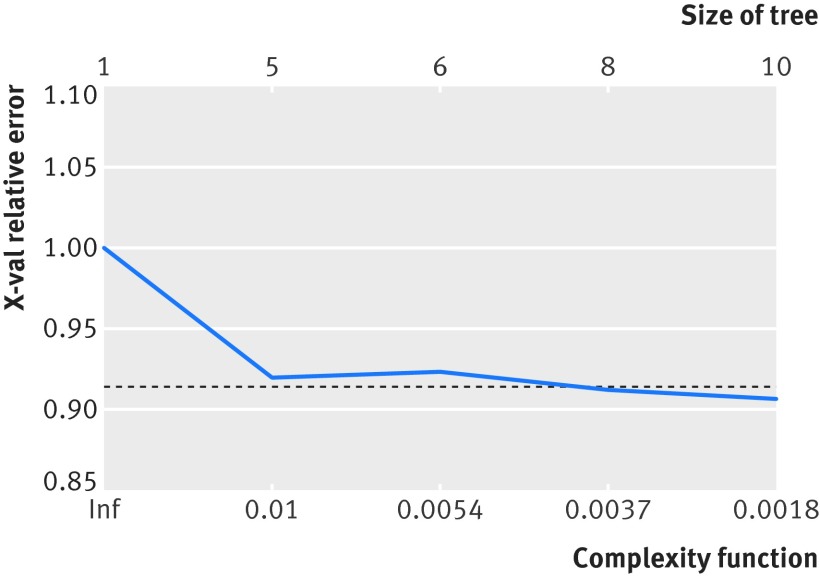
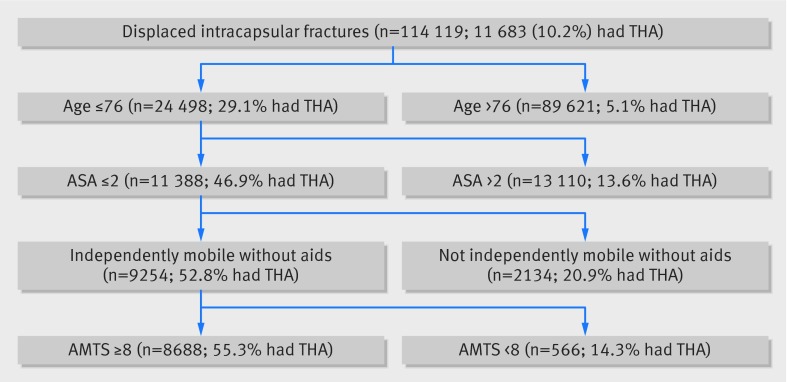
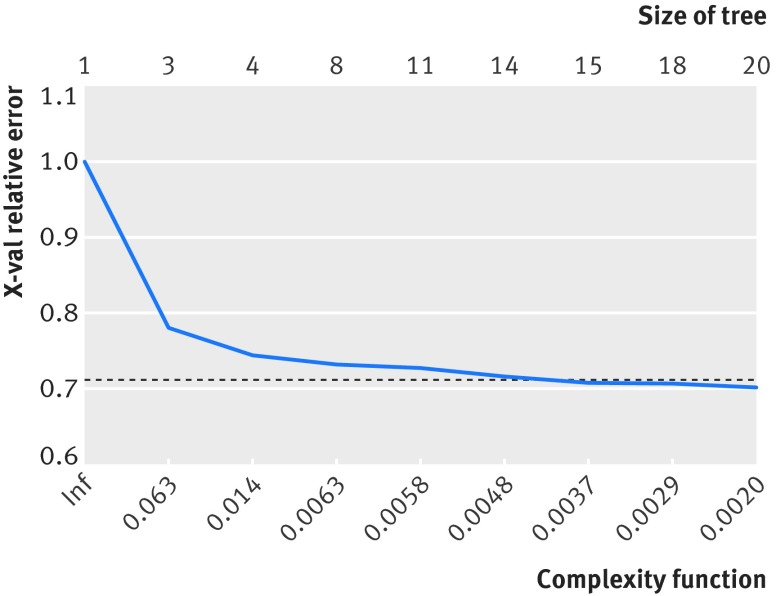
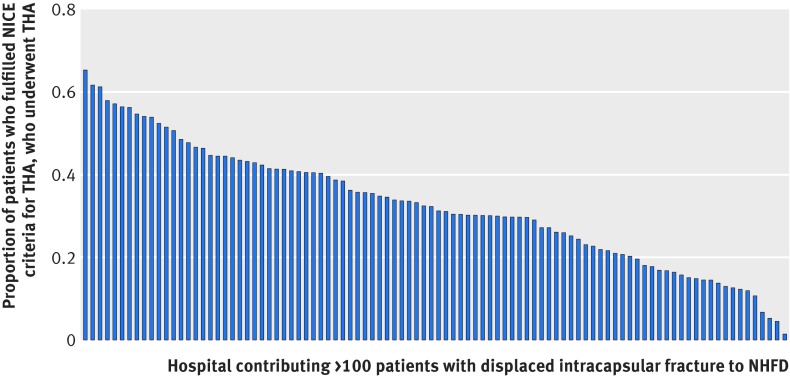
Results: 114 119 patients with hip fracture were included, 11 683 (10.2%) of whom underwent THA. Of those who satisfied the NICE criteria, 32% (6780) : received a THA. Of patients who underwent THA, 42% (4903) did not satisfy the NICE criteria. A recursive partitioning algorithm found that the NICE eligibility criteria did not optimally explain which patients underwent THA. A model with superior explanatory power drew distinctions that are not supported by NICE, which were an age cut off at 76 and a different ambulation cut off. Among patients who satisfied the NICE eligibility, the use of THA was less likely with higher age (odds ratio 0.88, 95% confidence interval 0.87 to 0.88), worsening abbreviated mental test scores (0.49 (0.41 to 0.58) for normal cognition v borderline cognitive impairment)), worsening American Society of Anesthesiologists score (0.74, 0.66 to 0.84), male sex (0.85, 0.77 to 0.93), worsening ambulatory status (0.32, 0.28 to 0.35 for walking with a stick v independent ambulation), and fifths of worsening socioeconomic area deprivation (0.76 (0.66 to 0.88) for least v most deprived fifth). Patients receiving treatment during the working week were more likely to receive THA than at the weekend (0.90, 0.83 to 0.98).
Conclusions: There are wide disparities in the use of THA among individuals with hip fractures, and compliance with NICE guidance is poor. Patients with higher levels of socioeconomic deprivation and those who require surgery at the weekend were less likely to receive THA. Inconsistent compliance with NICE recommendations means that the optimal treatment for older adults with hip fractures can depend on where and when they present to hospital.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Total hip arthroplasty after hip fracture.BMJ. 2016 Apr 27;353:i2217. doi: 10.1136/bmj.i2217. BMJ. 2016. PMID: 27121039 Free PMC article.
References
-
- Royal College of Physicians. National Hip Fracture Database annual report 2014. London, 2014.
-
- Burge RT, Worley D, Johansen A, et al. The cost of osteoporotic fractures in the UK: projections for 2000-2020. J Med Econ 2001;4:51-6210.3111/200104051062. - DOI
-
- Neuburger J, Currie C, Wakeman R, et al. The impact of a national clinician-led audit initiative on care and mortality after hip fracture in England: an external evaluation using time trends in non-audit data. Med Care 2015;53:686-91. 10.1097/MLR.0000000000000383 pmid:26172938. - DOI - PMC - PubMed
-
- Sahota O, Currie C. Hip fracture care: all change. Age Ageing 2008;37:128-9. 10.1093/ageing/afn007 pmid:18349006. - DOI - PubMed
-
- British Orthopaedic Association, British Geriatrics Society. The Care of Patients with Fragility Fracture.BOA, 2007.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous