

Fasting is not routinely required for determination of a lipid profile: clinical and laboratory implications including flagging at desirable concentration cut-points-a joint consensus statement from the European Atherosclerosis Society and European Federation of Clinical Chemistry and Laboratory Medicine
- PMID: 27122601
- PMCID: PMC4929379
- DOI: 10.1093/eurheartj/ehw152
Fasting is not routinely required for determination of a lipid profile: clinical and laboratory implications including flagging at desirable concentration cut-points-a joint consensus statement from the European Atherosclerosis Society and European Federation of Clinical Chemistry and Laboratory Medicine
Abstract
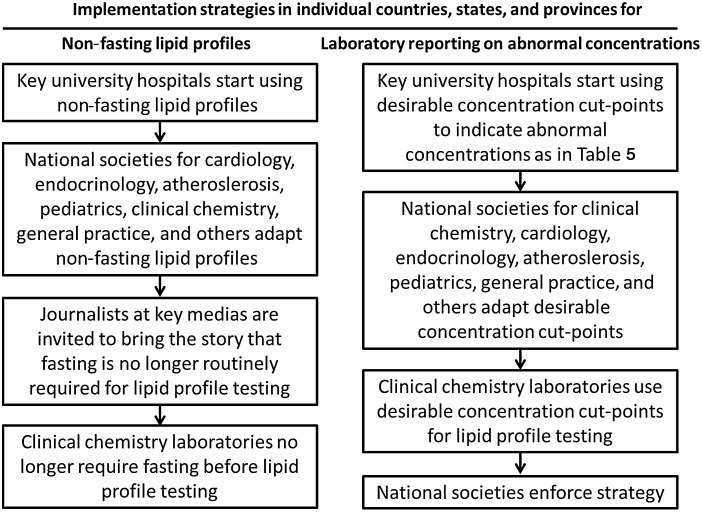
Aims: To critically evaluate the clinical implications of the use of non-fasting rather than fasting lipid profiles and to provide guidance for the laboratory reporting of abnormal non-fasting or fasting lipid profiles.
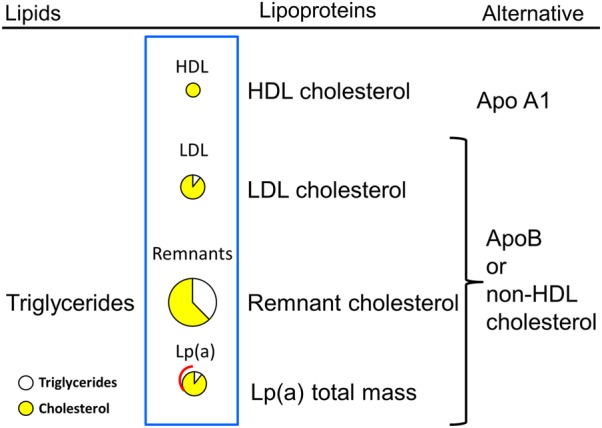
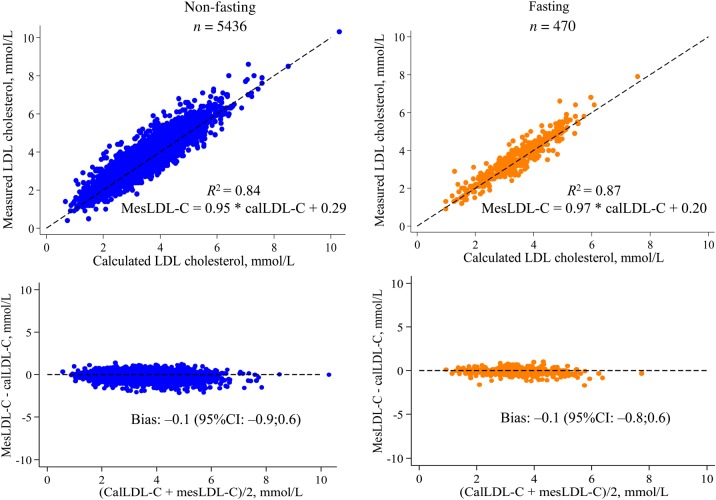
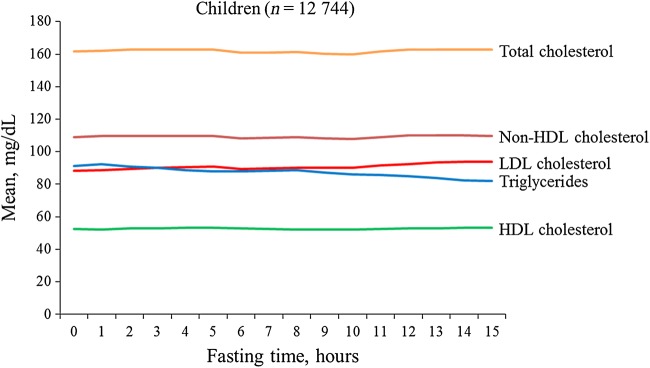
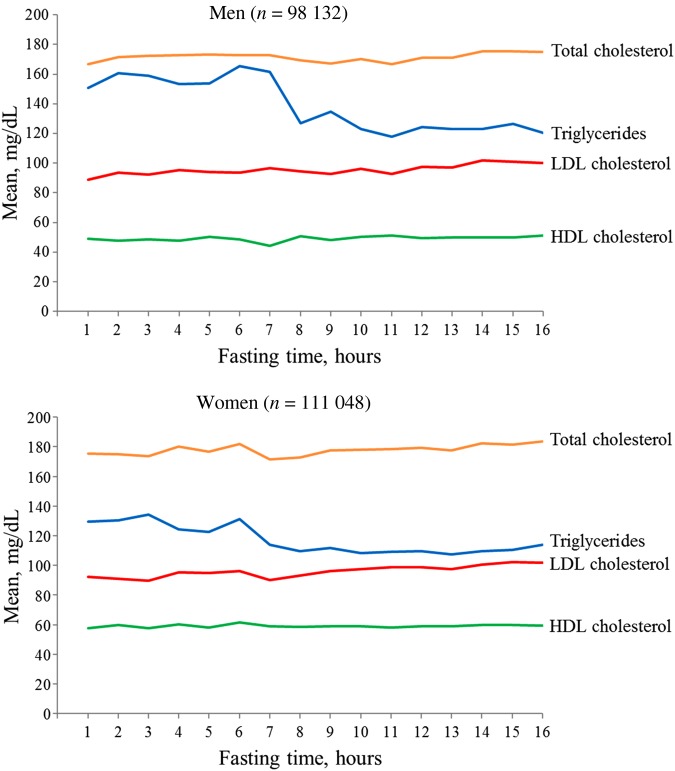
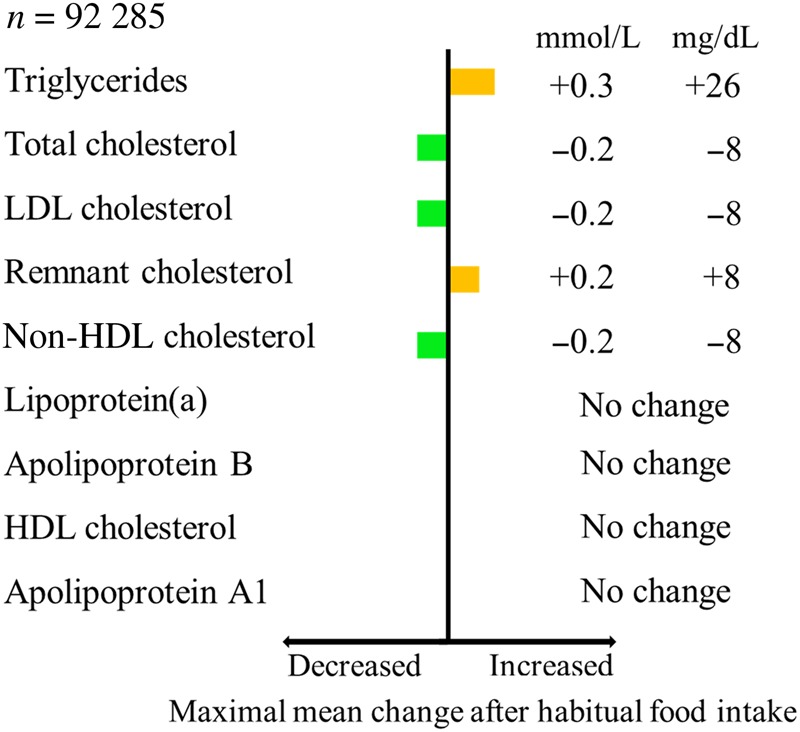
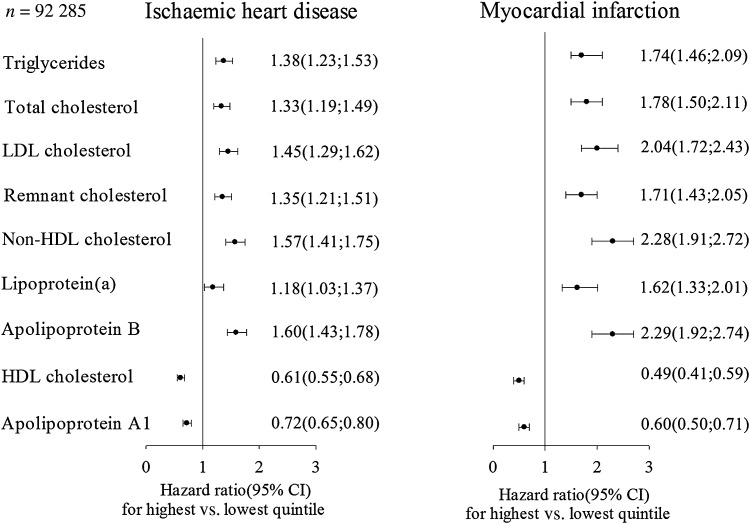
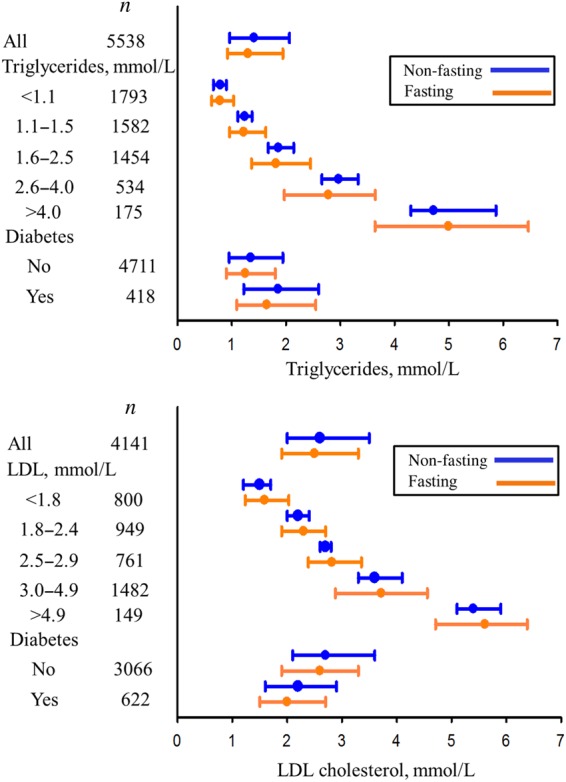
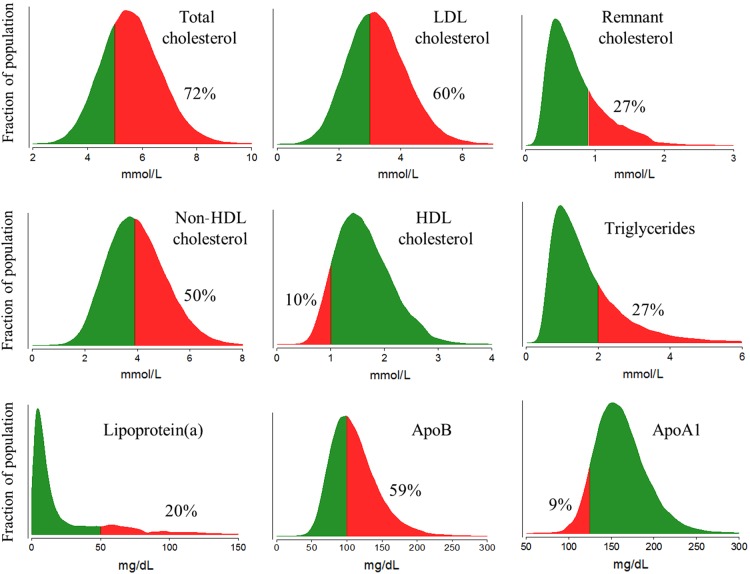
Methods and results: Extensive observational data, in which random non-fasting lipid profiles have been compared with those determined under fasting conditions, indicate that the maximal mean changes at 1-6 h after habitual meals are not clinically significant [+0.3 mmol/L (26 mg/dL) for triglycerides; -0.2 mmol/L (8 mg/dL) for total cholesterol; -0.2 mmol/L (8 mg/dL) for LDL cholesterol; +0.2 mmol/L (8 mg/dL) for calculated remnant cholesterol; -0.2 mmol/L (8 mg/dL) for calculated non-HDL cholesterol]; concentrations of HDL cholesterol, apolipoprotein A1, apolipoprotein B, and lipoprotein(a) are not affected by fasting/non-fasting status. In addition, non-fasting and fasting concentrations vary similarly over time and are comparable in the prediction of cardiovascular disease. To improve patient compliance with lipid testing, we therefore recommend the routine use of non-fasting lipid profiles, while fasting sampling may be considered when non-fasting triglycerides >5 mmol/L (440 mg/dL). For non-fasting samples, laboratory reports should flag abnormal concentrations as triglycerides ≥2 mmol/L (175 mg/dL), total cholesterol ≥5 mmol/L (190 mg/dL), LDL cholesterol ≥3 mmol/L (115 mg/dL), calculated remnant cholesterol ≥0.9 mmol/L (35 mg/dL), calculated non-HDL cholesterol ≥3.9 mmol/L (150 mg/dL), HDL cholesterol ≤1 mmol/L (40 mg/dL), apolipoprotein A1 ≤1.25 g/L (125 mg/dL), apolipoprotein B ≥1.0 g/L (100 mg/dL), and lipoprotein(a) ≥50 mg/dL (80th percentile); for fasting samples, abnormal concentrations correspond to triglycerides ≥1.7 mmol/L (150 mg/dL). Life-threatening concentrations require separate referral when triglycerides >10 mmol/L (880 mg/dL) for the risk of pancreatitis, LDL cholesterol >13 mmol/L (500 mg/dL) for homozygous familial hypercholesterolaemia, LDL cholesterol >5 mmol/L (190 mg/dL) for heterozygous familial hypercholesterolaemia, and lipoprotein(a) >150 mg/dL (99th percentile) for very high cardiovascular risk.
Conclusion: We recommend that non-fasting blood samples be routinely used for the assessment of plasma lipid profiles. Laboratory reports should flag abnormal values on the basis of desirable concentration cut-points. Non-fasting and fasting measurements should be complementary but not mutually exclusive.
Keywords: Cardiovascular disease; Lipids; Lipoproteins; Normal values; Reference values; Stroke.
© The Author 2016. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Rifai N, Warnick GR. Lipids, lipoproteins, apolipoproteins, and other cardiovascular risk factors. In: Burtis CA, Ashwood ER, Bruns DE, (eds), Tietz Textbook of Clinical Chemistry and Molecular Diagnostics, 4th ed Philadelphia: Elsevier Saunders; 2006, p903–982.
-
- Simundic AM, Cornes M, Grankvist K, Lippi G, Nybo M. Standardization of collection requirements for fasting samples: for the Working Group on Preanalytical Phase (WG-PA) of the European Federation of Clinical Chemistry and Laboratory Medicine (EFLM). Clin Chim Acta 2014;432:33–37. - PubMed
-
- Langsted A, Freiberg JJ, Nordestgaard BG. Fasting and nonfasting lipid levels: influence of normal food intake on lipids, lipoproteins, apolipoproteins, and cardiovascular risk prediction. Circulation 2008;118:2047–2056. - PubMed
-
- Watts GF, Cohn JS. Whither the lipid profile: feast, famine, or no free lunch? Clin Chem 2011;57:363–365. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
