

Early Elevated B-Type Natriuretic Peptide Levels are Associated with Cardiac Dysfunction and Poor Clinical Outcome in Pediatric Septic Patients
- PMID: 27122912
- PMCID: PMC4804972
- DOI: 10.6515/acs20141201e
Early Elevated B-Type Natriuretic Peptide Levels are Associated with Cardiac Dysfunction and Poor Clinical Outcome in Pediatric Septic Patients
Abstract
Background: To determine the B-type natriuretic peptide (BNP) level in pediatric septic patients, and to investigate its association with cardiovascular dysfunction and clinical outcome.
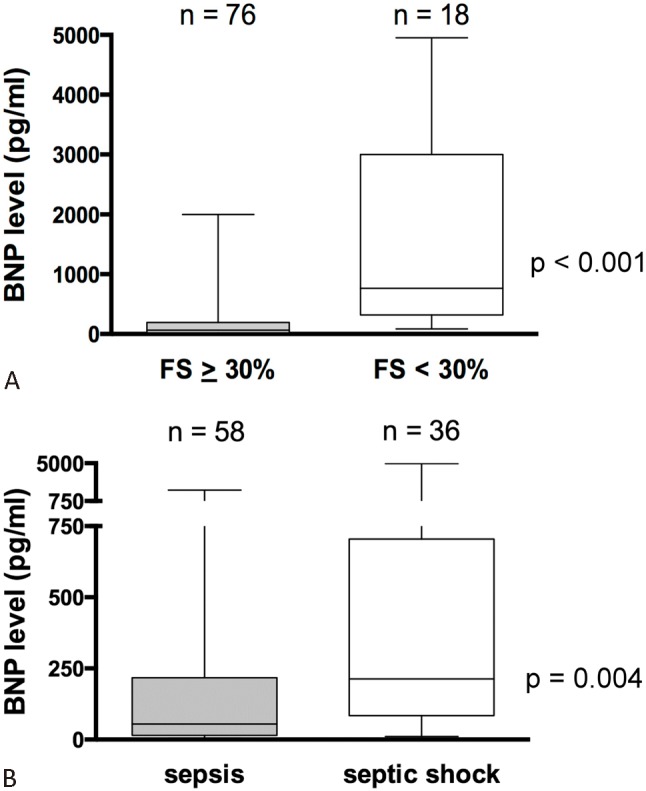
Methods: Pediatric patients with sepsis or septic shock were prospectively enrolled in our pediatric intensive care unit (PICU). On day 1 of admission, plasma BNP levels were measured at the time-point of echocardiography. Myocardial dysfunction was defined as left ventricular fractional shortening (FS) < 30%. Inotropic support was quantified by inotropic scores and disease severity was assessed by Pediatric Risk of Mortality (PRISM) III scores. Therafter, associations between BNP levels and clinical parameters were analyzed.
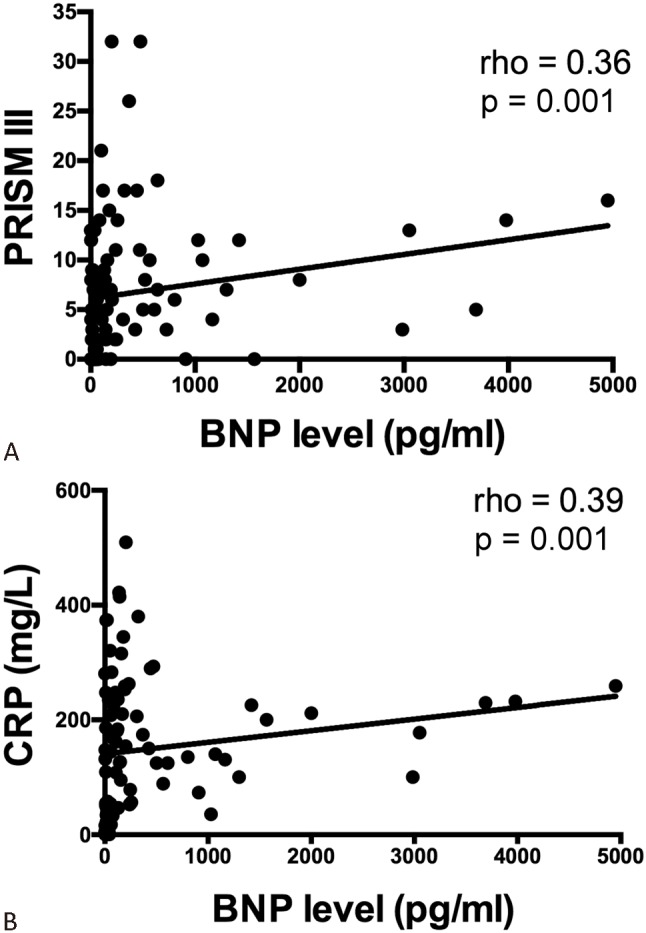
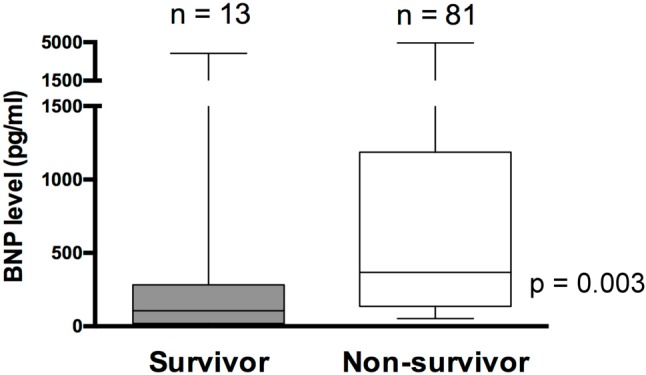
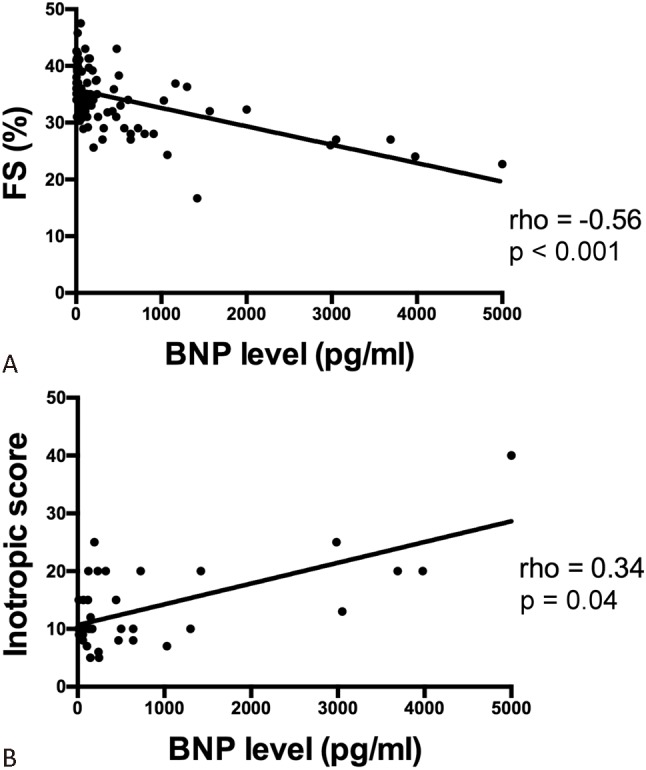
Results: There were 94 patients (mean: 5.6 yr, range: 2 mo-17 yr) that were consecutively enrolled in this study. The median BNP level was 127 pg/ml (range: 5 to 4950 pg/ml). BNP levels were correlated with PRISM III (rho = 0.36, p = 0.001) and C-reactive protein level (r = 0.39, p = 0.001). The median BNP levels were not only higher in patients with septic shock (n = 34) than those with sepsis (n = 58) (213 vs. 54 pg/ml, p = 0.0004), but also higher in patients with myocardial dysfunction (n = 18) than those with preserved myocardial function (n = 66) (765 vs. 65 pg/ml, p < 0.001). We also found that BNP levels correlated negatively with FS (r = -0.56, p < 0.001) and positively with inotropic scores (r = 0.34, p = 0.04). Most importantly, the median BNP levels were higher in non-survivors (n = 13) than survivors (n = 81) (367 vs. 106 pg/ml, p = 0.003).
Conclusions: BNP levels are elevated in pediatric septic patients early in the disease course, and increased levels are associated with cardiovascular dysfunction and worse clinical outcome.
Key words: B-type natriuretic peptide; Cardiac function; Pediatric; Sepsis; Septic shock.
Figures
Similar articles
-
Plasma brain natriuretic peptide and troponin levels in severe sepsis and septic shock: relationships with systolic myocardial dysfunction and intensive care unit mortality.J Intensive Care Med. 2014 Jul-Aug;29(4):229-37. doi: 10.1177/0885066612471621. Epub 2013 Jan 1. J Intensive Care Med. 2014. PMID: 23753226
-
B-type natriuretic peptide as a marker for sepsis-induced myocardial depression in intensive care patients.Crit Care Med. 2008 Nov;36(11):3030-7. doi: 10.1097/CCM.0b013e31818b9153. Crit Care Med. 2008. PMID: 18824903
-
Elevation of brain natriuretic peptide levels in children with septic shock.Pediatr Crit Care Med. 2008 Sep;9(5):478-83. doi: 10.1097/PCC.0b013e3181849b99. Pediatr Crit Care Med. 2008. PMID: 18679143
-
The utility of brain natriuretic peptides in septic shock as markers for mortality and cardiac dysfunction: A systematic review.Int J Clin Pract. 2019 Jul;73(7):e13374. doi: 10.1111/ijcp.13374. Epub 2019 Jun 17. Int J Clin Pract. 2019. PMID: 31111653
-
Brain natriuretic peptide: a potential marker for mortality in septic shock.Int J Infect Dis. 2004 Sep;8(5):271-4. doi: 10.1016/j.ijid.2003.12.007. Int J Infect Dis. 2004. PMID: 15325595 Review.
Cited by
-
What Is High Enough? Elevated NT-pro-BNP in Decompensated Paroxysmal Supraventricular Tachycardia.J Pediatr Intensive Care. 2018 Mar;7(1):49-53. doi: 10.1055/s-0037-1603760. Epub 2017 Jun 12. J Pediatr Intensive Care. 2018. PMID: 31073468 Free PMC article.
-
Elevated High-Sensitivity Troponin and NT-proBNP Values in Febrile Children.Pediatr Emerg Care. 2024 Feb 1;40(2):108-113. doi: 10.1097/PEC.0000000000003097. Epub 2023 Dec 20. Pediatr Emerg Care. 2024. PMID: 38113471 Free PMC article.
-
Sepsis: Precision-Based Medicine for Pregnancy and the Puerperium.Int J Mol Sci. 2019 Oct 29;20(21):5388. doi: 10.3390/ijms20215388. Int J Mol Sci. 2019. PMID: 31671794 Free PMC article. Review.
-
Cardiac Biomarkers in Pediatrics: An Undervalued Resource.Clin Chem. 2021 Jul 6;67(7):947-958. doi: 10.1093/clinchem/hvab063. Clin Chem. 2021. PMID: 34125147 Free PMC article. Review.
-
The effect of myocardial dysfunction on mortality in children with septic shock: a prospective observational study.Eur J Pediatr. 2023 Oct;182(10):4759-4766. doi: 10.1007/s00431-023-05236-1. Epub 2023 Oct 4. Eur J Pediatr. 2023. PMID: 37792091
References
-
- Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101:1644–1655. - PubMed
-
- Kutko MC, Calarco MP, Flaherty MB, et al. Mortality rates in pediatric septic shock with and without multiple organ system failure. Pediatr Crit Care Med. 2003;4:333–337. - PubMed
-
- Parrillo JE, Parker MM, Natanson C, et al. Septic shock in humans: advances in the understanding of pathogenesis, cardiovascular dysfunction, and therapy. Ann Intern Med. 1990;113:227–242. - PubMed
-
- Hsu JH, Wu JR, Dai ZK, et al. Cardiac Arrhythmias - New Considerations, 1st ed. Croatia, InTech: In: Breijo-Marquez FR, Ed.; 2012. Approach to ventricular arrhythmias in the pediatric intensive care unit; p. DOI: 10.5772/25402.
-
- Krishnagopalan S, Kumar A, Parrillo JE, Kumar A. Myocardial dysfunction in the patient with sepsis. Curr Opin Crit Care. 2002;8:376–388. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials