

Review
doi: 10.5173/ceju.2016.605b.
Epub 2015 Nov 20.
Tips and tricks of ureteroscopy: consensus statement. Part II. Advanced ureteroscopy
Affiliations
- PMID: 27123335
- PMCID: PMC4846730
- DOI: 10.5173/ceju.2016.605b
Item in Clipboard
Review
Tips and tricks of ureteroscopy: consensus statement. Part II. Advanced ureteroscopy
Cent European J Urol.
2016.
Abstract
Our "tips and tricks" focuses on all aspects of upper tract endourology and we hope these will be of use to all trainees and consultants who perform ureteroscopy. We report an "expert consensus view" from experienced endourological surgeons, on all aspects of advanced ureteroscopic techniques, with a particular focus on avoiding and getting out of trouble while performing ureteroscopy. In this paper we provide a summary of placing ureteric access sheath, flexible ureteroscopy, intra renal stone fragmentation and retrieval, maintaining visual clarity and biopsy of ureteric and pelvicalyceal tumours.
Keywords: stent; ureterorenoscopy; ureteroscopy; urolithiasis.
Figures
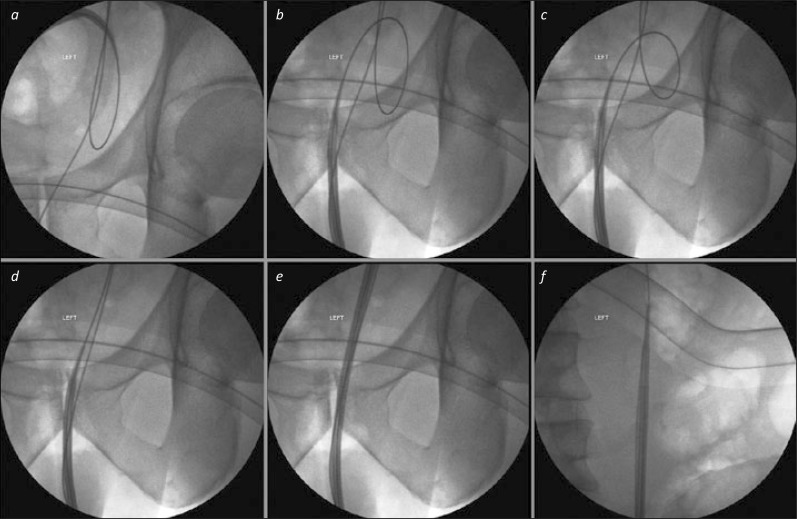
Wire problems (in bladder) for access sheath insertion. 1a. A straight safety wire is present, but the working wire, over which the access sheath is being passed, is substantially coiled in the bladder. Further advancement of the sheath will not only fail to access the ureter, but is likely to result in displacement of the working wire to the bladder. 1b. The access sheath has been withdrawn to the urethra. 1c. The working guide wire has been withdrawn slightly, such that the coiled loop is of smaller diameter. 1d. The working wire is now straight, and the tip of the access sheath has been moved along it towards the left ureteric orifice. 1e. Keeping the image intensifier over the lower third of the ureter, the access sheath can be advanced under fluoroscopic control to ensure there is no “buckling” in this part of the ureter. 1f. Once the lower third has been successfully traversed, the image intensifier can be moved to the proximal ureter to allow precise positioning of the tip of the sheath in the upper ureter.
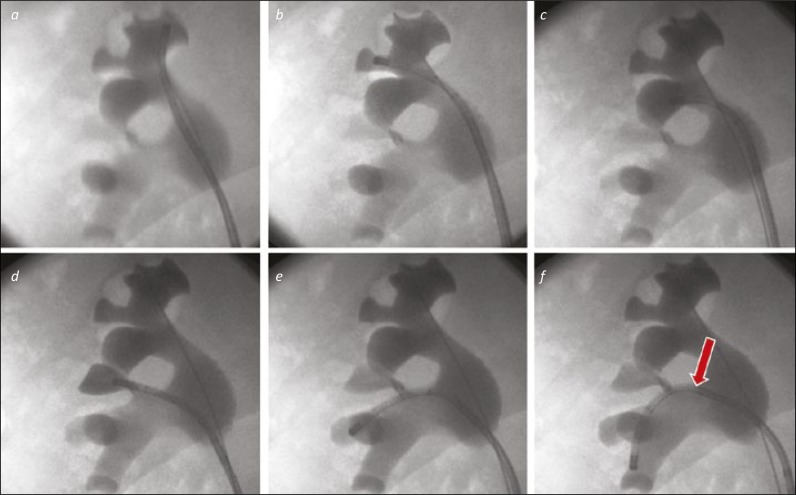
A “Complete Tour” of the right kidney. 2a. The ureterorenoscope is directed to the upper medial calyx as the starting point for an anti-clockwise tour of the collecting system. 2b. The upper middle calyx will be visualised (where the safety wire is located) as the scope is moved to the upper lateral calyx. 2c. The scope is seen in the posterior upper pole calyx. 2d. The interpole, not well seen on the images 3a-c is filled with contrast via the scope to confirm it has been visualised. 2e. The scope is placed in the next calyces down, in the lateral part of the lower pole. Both calyces can be inspected in turn before moving to the lowermost calyx. 2f. The ureterorenoscope is deflected into the lower medial calyx. This required use of the secondary (passive) deflection from the renal pelvis / infundibulum to the interpole (arrow).
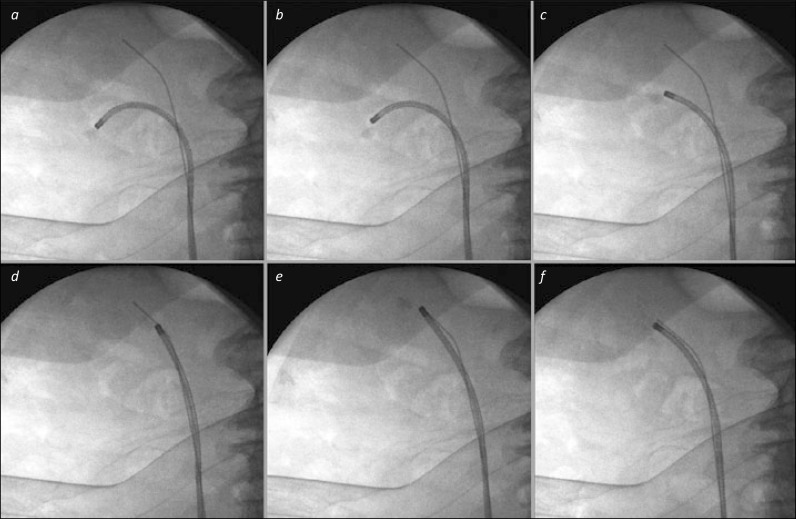
Basket relocation of lower pole stone. 3a. The stone has been identified in the lower pole, and is grasped in a basket to prepare for relocation. 3b and c. The ureterorenoscope is manoeuvred out of the lower calyx towards the renal pelvis. 3d. The scope is advanced into the patient to the upper pole – the presence of the safety wire in the upper calyx can aid this both under endoscopic and fluoroscopic control. 3e. The stone is then released from the basket, which is withdrawn from the scope, and replaced with an appropriate laser fibre for stone fragmentation. 3f. The stone has been successfully broken into small pieces. It will be easier to re-pass the ureterorenoscope back and forth to this upper calyx for basket stone retrieval than to direct it repeatedly to the lower calyx where the stone was originally, particularly as the safety wire “guides the way”.
References
-
- Turney BW, Reynard JM, Noble JG, Keoghane SR. Trends in urological stone disease. BJU Int. 2012;109:1082–1087. - PubMed
-
- Ulvik Ø, Rennesund K, Gjengstø P, Wentzel-Larsen T, Ulvik NM. Ureteroscopy with and without safety guide wire: should the safety wire still be mandatory? J Endourol. 2013;27:1197–1202. - PubMed
-
- Dickstein RJ, Kreshover JE, Babayan RK, Wang DS. Is a safety wire necessary during routine flexible ureteroscopy? J Endourol. 2010;24:1589–1592. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources