

Paroxysmal hypnogenic dyskinesia is associated with mutations in the PRRT2 gene
- PMID: 27123484
- PMCID: PMC4830198
- DOI: 10.1212/NXG.0000000000000066
Paroxysmal hypnogenic dyskinesia is associated with mutations in the PRRT2 gene
Abstract
Objective: To explore the potential causative genes of paroxysmal hypnogenic dyskinesia (PHD), which was initially considered a subtype of paroxysmal dyskinesia and has been recently considered a form of nocturnal frontal lobe epilepsy (NFLE).
Methods: Eleven patients with PHD were recruited. Mutations in proline-rich region transmembrane protein-2 (PRRT2), myofibrillogenesis regulator 1 (MR-1), solute carrier family 2, member 1 (SLC2A1), calcium-activated potassium channel alpha subunit (KCNMA1), cholinergic receptor, nicotinic, alpha 4 (CHRNA4), cholinergic receptor, nicotinic, beta 2 (CHRNB2), cholinergic receptor, nicotinic, alpha 2 (CHRNA2), and potassium channel subfamily T member 1 (KCNT1) were screened by direct sequencing.
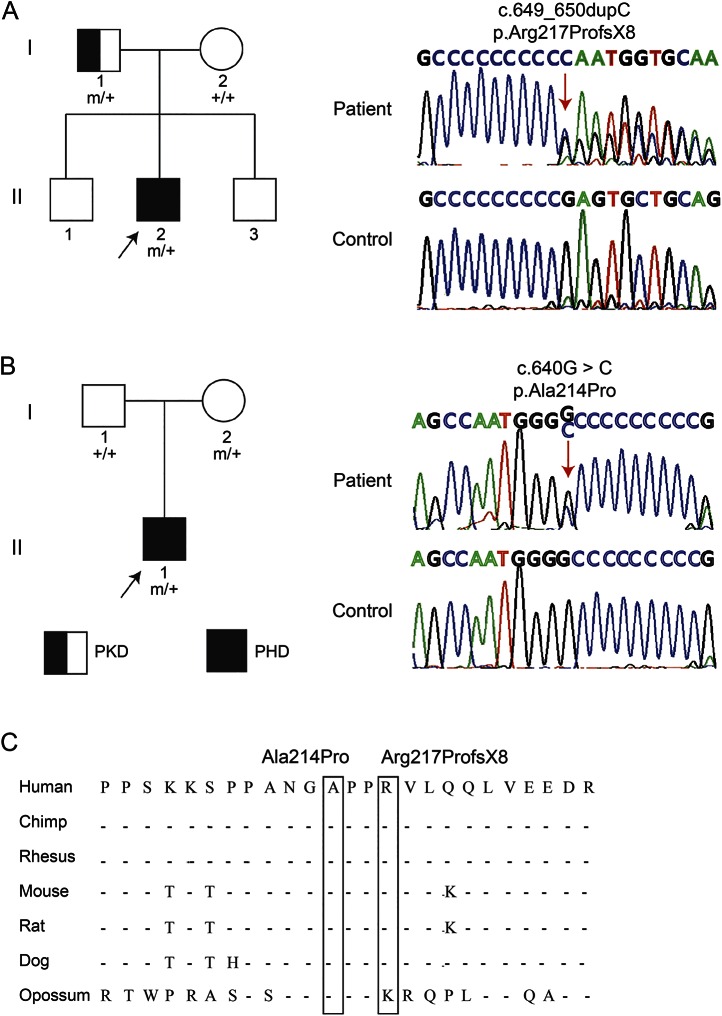
Results: Two PRRT2 mutations were identified in patients with typical PHD. A mutation of c.649dupC (p.Arg217ProfsX8) was identified in a patient with PHD and his father who was diagnosed with paroxysmal kinesigenic dyskinesia. An additional mutation of c.640G>C (p.Ala214Pro) was identified in a sporadic patient and his asymptomatic mother. No mutations were found in the other screened genes.
Conclusions: The present study identified PRRT2 mutations in PHD, extending the phenotypic spectrum of PRRT2 and supporting the classification of PHD as a subtype of paroxysmal dyskinesia but not NFLE. Based on the results of this study, screening for the PRRT2 mutation is recommended in patients with PHD.
Figures
References
-
- Lugaresi E, Cirignotta F. Hypnogenic paroxysmal dystonia: epileptic seizure or a new syndrome? Sleep 1981;4:129–138. - PubMed
-
- Lee BI, Lesser RP, Pippenger CE, et al. Familial paroxysmal hypnogenic dystonia. Neurology 1985;35:1357–1360. - PubMed
-
- Demirkiran M, Jankovic J. Paroxysmal dyskinesias: clinical features and classification. Ann Neurol 1995;38:571–579. - PubMed
-
- Bhatia KP, Schneider SA. Identification of PRRT2 as the causative gene of paroxysmal kinesigenic dyskinesia. Mov Disord 2012;27:707. - PubMed
-
- Liu XR, Wu M, He N, et al. Novel PRRT2 mutations in paroxysmal dyskinesia patients with variant inheritance and phenotypes. Genes Brain Behav 2013;12:234–240. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous