

Roux-en-Y Gastric Bypass Versus Medical Treatment for Type 2 Diabetes Mellitus in Obese Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 27124041
- PMCID: PMC4998704
- DOI: 10.1097/MD.0000000000003462
Roux-en-Y Gastric Bypass Versus Medical Treatment for Type 2 Diabetes Mellitus in Obese Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
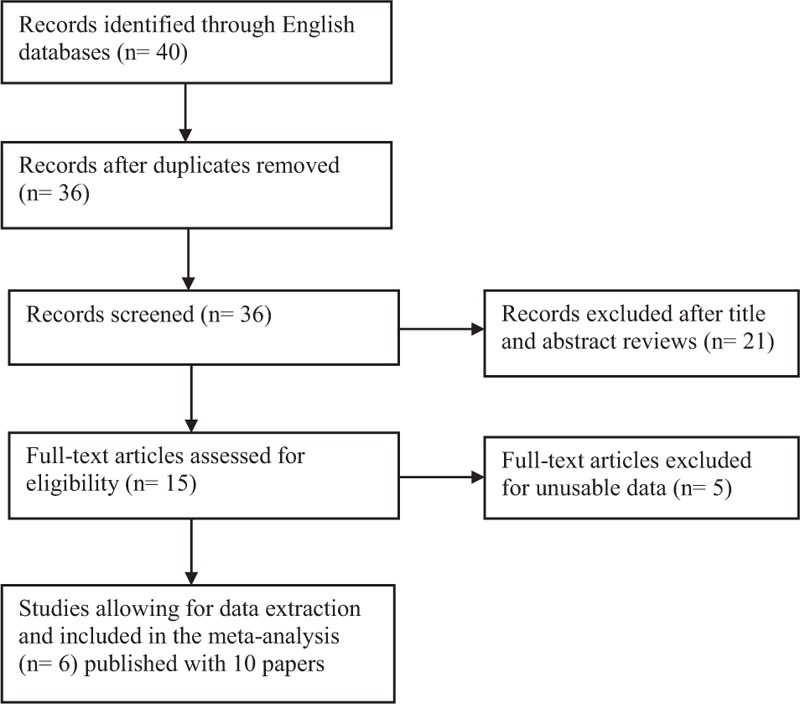
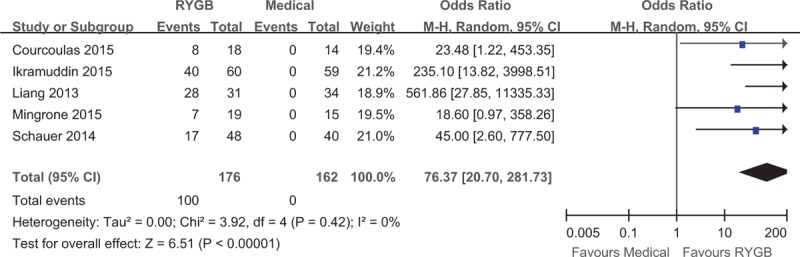
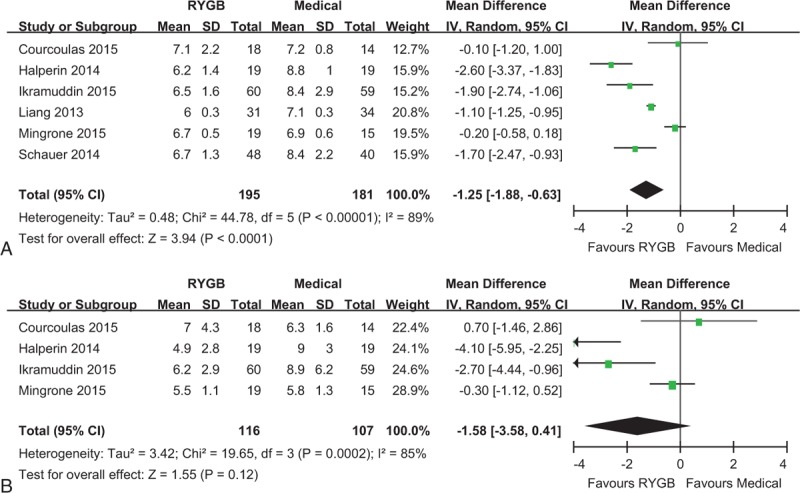
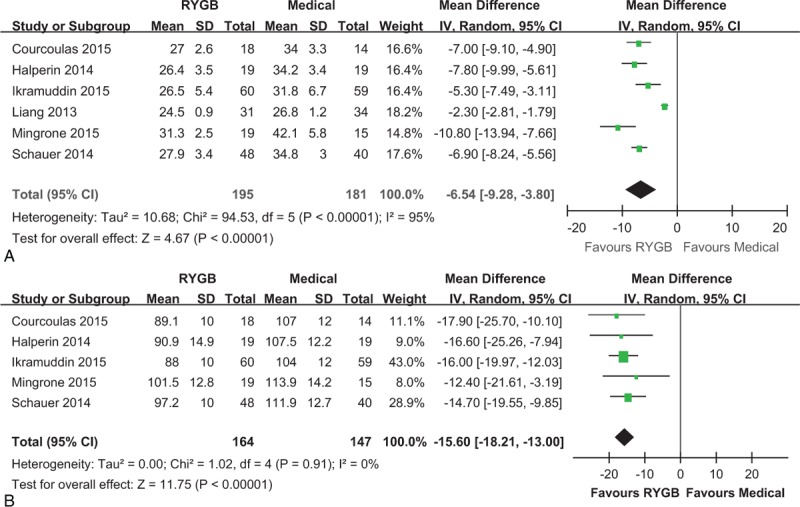
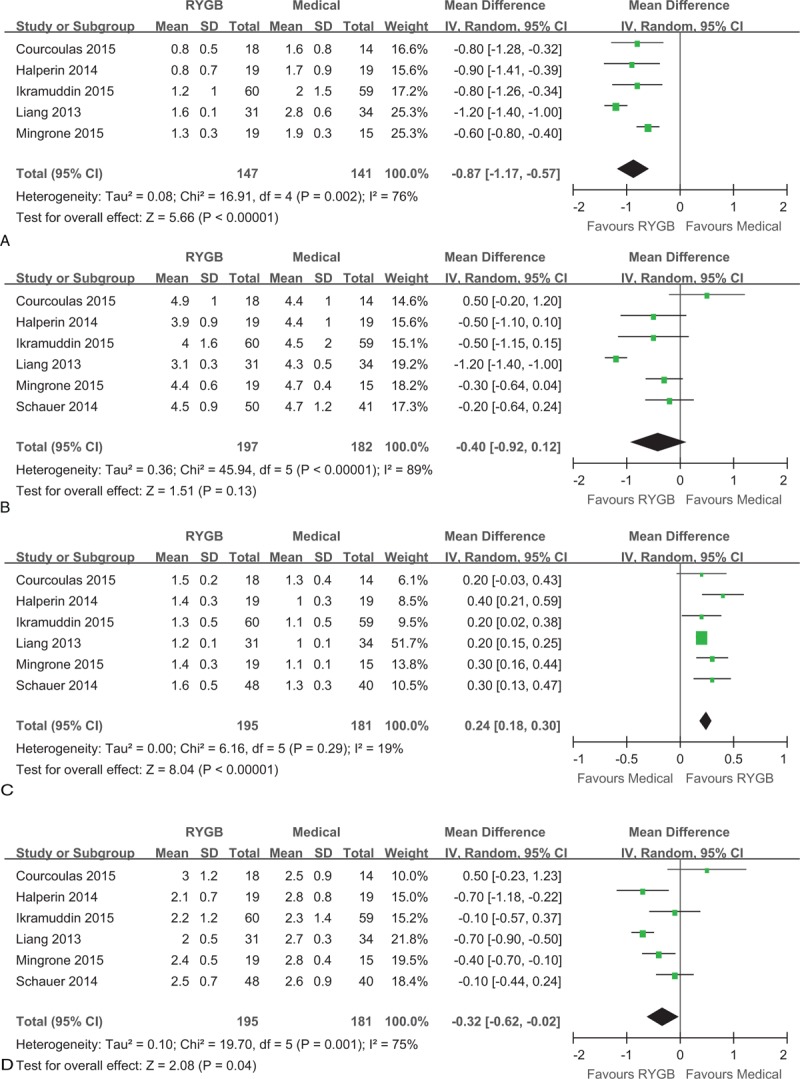
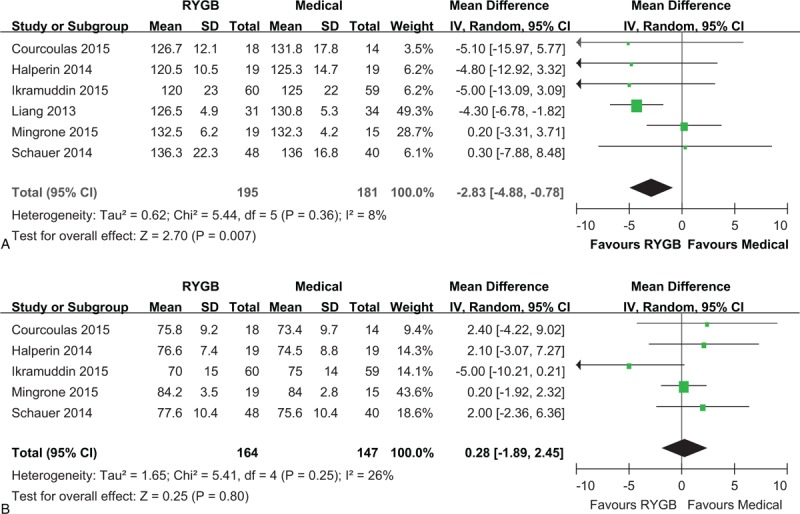
The aim of the study is to compare Roux-en-Y gastric bypass (RYGB) surgery versus medical treatment for type 2 diabetes mellitus (T2DM) in obese patients.Bariatric surgery can achieve remission of T2DM in obese patients. RYGB surgery has been performed as one of the most common surgical treatment options for obese patients with T2DM, but the efficacy of RYGB surgery comparing with medical treatment alone has not been conclusively determined.A systematic literature search identified randomized controlled trials (RCTs) evaluating RYGB surgery versus medical treatment for T2DM in obese patients was conducted in PubMed, Embase, Cochrane Database, and Cochrane Clinical Trials Registry. This systematic review and meta-analysis were performed according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. The primary outcome was T2DM remission. Additional analyses comprised hemoglobin A1c (HbA1c), fasting plasma glucose (FPG), body mass index (BMI), waist circumference, serum lipid level, blood pressure, medication use, and adverse events. Random-effects meta-analyses were calculated and presented as weighted odds ratio (OR) or mean difference (MD) with 95% confidence intervals (CI).Six RCTs concerning 410 total obese T2DM patients were included. Follow-up ranged from 12 to 60 months. RYGB surgery was associated with a higher T2DM remission rate (OR: 76.37, 95% CI: 20.70-281.73, P < 0.001) and serum level of high-density lipoprotein cholesterol (MD: 0.24 mmol/L, 95% CI 0.18-0.30 mmol/L, P < 0.001) than medical treatment alone. HbA1c (MD: -1.25%, 95% CI: -1.88% to -0.63%, P < 0.001), BMI (MD: -6.54 kg/m, 95% CI: -9.28 to -3.80 kg/m, P < 0.001), waist circumference (MD: -15.60 cm, 95% CI: -18.21 to -13.00 cm, P < 0.001), triglyceride (MD: -0.87 mmol/L, 95% CI: -1.17 to -0.57 mmol/L, P < 0.001), low-density lipoprotein cholesterol (MD: -0.32 mmol/L, 95% CI: -0.62 to -0.02 mmol/L, P = 0.04), systolic blood pressure (MD: -2.83 mm Hg, 95% CI: -4.88 to -0.78 mm Hg, P < 0.01) were lower after RYGB surgery. However, FPG (MD: -1.58 mmol/L, 95% CI: -3.58 to 0.41 mmol/L, P = 0.12), total cholesterol (MD: -0.40 mmol/L, 95% CI: -0.92 to 0.12 mmol/L, P = 0.13), and diastolic blood pressure (MD: 0.28 mm Hg, 95% CI: -1.89 to 2.45 mm Hg, P = 0.80) were not significantly different between the 2 treatment groups. The medicine use and quality of life were solely improved in the surgical group. Nutritional deficiencies and anemia were noted more frequently in the RYGB group.RYGB surgery is superior to medical treatment for short- to medium-term remission of T2DM, improvement of metabolic condition, and cardiovascular risk factors. Further RCTs should address the safety and long-term benefits of RYGB surgery on obese patients with T2DM.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Skinner AC, Skelton JA. Prevalence and trends in obesity and severe obesity among children in the United States, 1999–2012. JAMA Pediatrics 2014; 168:561–566. - PubMed
-
- Skrha J. Diabetes mellitus–a global pandemic. Keynote lecture presented at the Wonca conference in Prague in June 2013. Eur J Gen Pract 2014; 20:65–68. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
