

Frequency Dependence of Petechial Hemorrhage and Cardiomyocyte Injury Induced during Myocardial Contrast Echocardiography
- PMID: 27126240
- PMCID: PMC4912900
- DOI: 10.1016/j.ultrasmedbio.2016.03.017
Frequency Dependence of Petechial Hemorrhage and Cardiomyocyte Injury Induced during Myocardial Contrast Echocardiography
Abstract
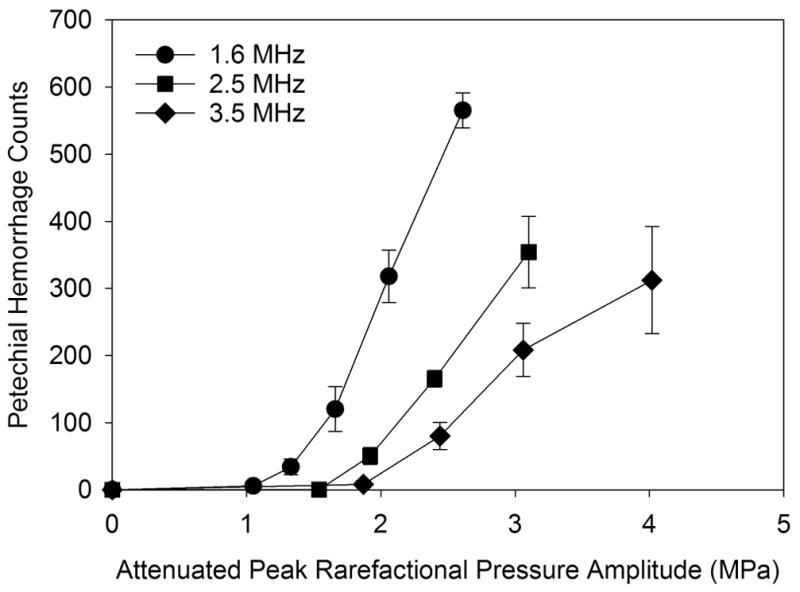
Myocardial contrast echocardiography (MCE) for perfusion imaging can induce microscale bio-effects during intermittent high-Mechanical Index scans. The dependence of MCE-induced bio-effects on the ultrasonic frequency was examined in rats at 1.6, 2.5 and 3.5 MHz. Premature complexes were counted in the electrocardiogram, petechial hemorrhages with microvascular leakage on the heart surface were observed at the time of exposure, plasma troponin elevation was measured after 4 h and cardiomyocyte injury was detected at 24 h. Increasing response to exposure above an apparent threshold was observed for all endpoints at each frequency. The effects decreased with increasing ultrasonic frequency, and the thresholds increased. Linear regressions for frequency-dependent thresholds indicated coefficients and exponents of 0.6 and 1.07 for petechial hemorrhages, respectively, and 1.02 and 0.8 for cardiomyocyte death, compared with 1.9 and 0.5 (square root) for the guideline limit of the mechanical index. The results clarify the dependence of cardiac bio-effects on frequency, and should allow development of theoretical descriptions of the phenomena and improved safety guidance for MCE.
Keywords: Cardiomyocyte injury; Diagnostic ultrasound adverse effects; Myocardial contrast echocardiography; Ultrasonic cavitation biology.
Copyright © 2016 World Federation for Ultrasound in Medicine & Biology. Published by Elsevier Inc. All rights reserved.
Figures













References
-
- Apfel RE, Holland CK. Gauging the likelihood of cavitation from short-pulse, low-duty cycle diagnostic ultrasound. Ultrasound Med Biol. 1991;17:179–85. - PubMed
-
- Chapman S, Windle J, Xie F, McGrain A, Porter TR. Incidence of cardiac arrhythmias with therapeutic versus diagnostic ultrasound and intravenous microbubbles. J Ultrasound Med. 2005;24:1099–1107. - PubMed
-
- Chen S, Kroll MH, Shohet RV, Frenkel P, Mayer SA, Grayburn PA. Bioeffects of myocardial contrast microbubble destruction by echocardiography. Echocardiography. 2002;19:495–500. - PubMed
-
- Church CC, Carstensen EL, Nyborg WL, Carson PL, Frizzell LA, Bailey MR. The risk of exposure to diagnostic ultrasound in postnatal subjects: nonthermal mechanisms. J Ultrasound Med. 2008;27:565–92. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
