

Uptake of antiretroviral therapy and male circumcision after community-based HIV testing and strategies for linkage to care versus standard clinic referral: a multisite, open-label, randomised controlled trial in South Africa and Uganda
- PMID: 27126488
- PMCID: PMC4852382
- DOI: 10.1016/S2352-3018(16)00020-5
Uptake of antiretroviral therapy and male circumcision after community-based HIV testing and strategies for linkage to care versus standard clinic referral: a multisite, open-label, randomised controlled trial in South Africa and Uganda
Abstract
Background: Male circumcision decreases HIV acquisition by 60%, and antiretroviral therapy (ART) almost eliminates HIV transmission from HIV-positive people who are virally suppressed; however, coverage of these interventions has lagged behind targets. We aimed to assess whether community-based HIV testing with counsellor support and point-of-care CD4 cell count testing would increase uptake of ART and male circumcision.
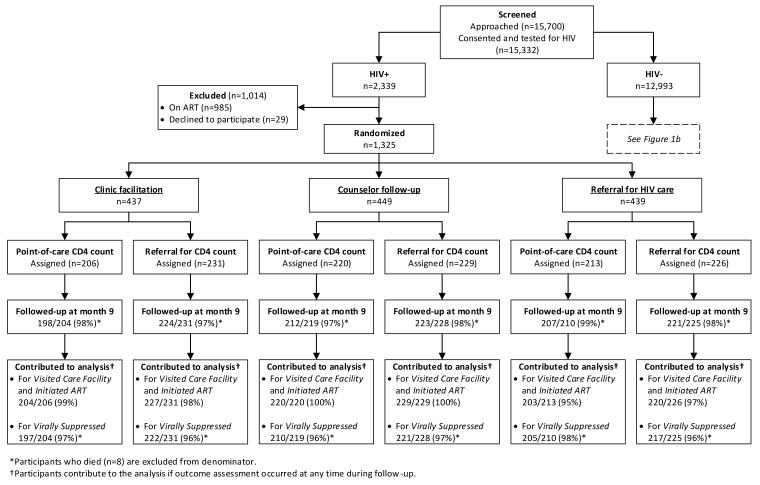
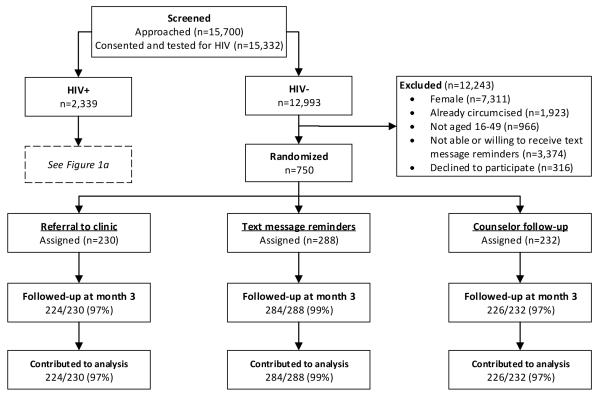
Methods: We did this multisite, open-label, randomised controlled trial in six research-naive communities in rural South Africa and Uganda. Eligible HIV-positive participants (aged ≥16 years) were randomly assigned (1:1:1) in a factorial design to receive lay counsellor clinic linkage facilitation, lay counsellor follow-up home visits, or standard-of-care clinic referral, and then (1:1) either point-of-care CD4 cell count testing or referral for CD4 testing. HIV-negative uncircumcised men (aged 16-49 years) who could receive secure mobile phone text messages were randomly assigned (1:1:1) to receive text message reminders, lay counsellor visits, or standard clinic referral. The study biostatistician generated the randomisation schedule via a computer-generated random number program with varying block sizes (multiples of six or three) stratified by country. Primary outcomes for HIV-positive people were obtaining a CD4 cell count, linkage to an HIV clinic, ART initiation, and viral suppression at 9 months, and for HIV-negative uncircumcised men were visiting a circumcision facility and uptake of male circumcision at 3 months. We assessed social harms as a safety outcome throughout the study. We did the primary analyses by intention to treat. This trial is registered with ClinicalTrials.gov, number NCT02038582.
Findings: Between June 6, 2013, and March 11, 2015, 15 332 participants were tested. 2339 (15%) participants tested HIV positive, of whom 1325 (57%) were randomly assigned to receive lay counsellor clinic linkage facilitation (n=437), lay counsellor follow-up home visits (n=449), or standard clinic referral (n=439), and then point-of-care CD4 cell testing (n=206, n=220, and n=213, respectively) or referral for CD4 testing (n=231, n=229, and n=226, respectively). 12 993 (85%) participants tested HIV negative, of whom 750 (6%) uncircumcised men were randomly assigned to receive clinic referral (n=230), text message reminders (n=288), or lay counsellor follow-up visits (n=232). 1218 (93%) of 1303 HIV-positive participants were linked to care, but only 488 (37%) participants initiated ART. Overall, 635 (50%) of 1272 HIV-positive individuals achieved viral suppression at 9 months: 219 (52%) of 419 participants in the clinic facilitation group, 202 (47%) of 431 participants in the lay counsellor follow-up group, and 214 (51%) of 422 participants in the clinic referral group, with no significant differences between groups (p=0·668 for clinic facilitation and p=0·273 for lay counsellor follow-up vs clinic referral). 523 (72%) of 734 HIV-negative men visited a circumcision facility, with no difference between groups. 62 (28%) of 224 men were circumcised in the male circumcision clinic referral group compared with 137 (48%) of 284 men in the text message reminder group (relative risk 1·72, 95% CI 1·36-2·17; p<0·0001) and 106 (47%) of 226 men in the lay counsellor follow-up group (1·67, 1·29-2·14; p=0·0001). No cases of study-related social harm were reported, including probing about partnership separation, unintended disclosure, gender-based violence, and stigma.
Interpretation: All the community-based strategies achieved high rates of linkage of HIV-positive people to HIV clinics, roughly a third of whom initiated ART, and of those more than 80% were virally suppressed at 9 months. Uptake of male circumcision was almost two-times higher in men who received text message reminders or lay counsellor visits than in those who received standard-of-care clinic referral. Clinic barriers to ART initiation should be addressed in future strategies to increase the proportion of HIV-positive people accessing treatment and achieving viral suppression.
Funding: National Institute of Allergy and Infectious Diseases, National Institutes of Health.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Linkage to care: a step on the path, but not the destination.Lancet HIV. 2016 May;3(5):e193-4. doi: 10.1016/S2352-3018(16)00038-2. Epub 2016 Mar 10. Lancet HIV. 2016. PMID: 27126481 No abstract available.
References
-
- Geldsetzer P, Bloom D, Humair S, Bärnighausen T. Copenhagen Consensus Perspective Paper Health - HIV/AIDS: Benefits and costs of the HIV/AIDS targets for the post-2015 development agenda. Copenhagen Consensus Center; Frederiksberg, Denmark: 2015.
-
- Anderson S, Cherutich P, Kilonzo N, et al. Maximising the Impact of Combination HIV Prevention through Prioritising the People and Places in Greatest Need. Lancet. 2014 - PubMed
-
- Bailey RC, Moses S, Parker CB, et al. Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. Lancet. 2007;369(9562):643–56. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
