

Intratracheal Gene Delivery of SERCA2a Ameliorates Chronic Post-Capillary Pulmonary Hypertension: A Large Animal Model
- PMID: 27126531
- PMCID: PMC6019268
- DOI: 10.1016/j.jacc.2016.02.049
Intratracheal Gene Delivery of SERCA2a Ameliorates Chronic Post-Capillary Pulmonary Hypertension: A Large Animal Model
Abstract
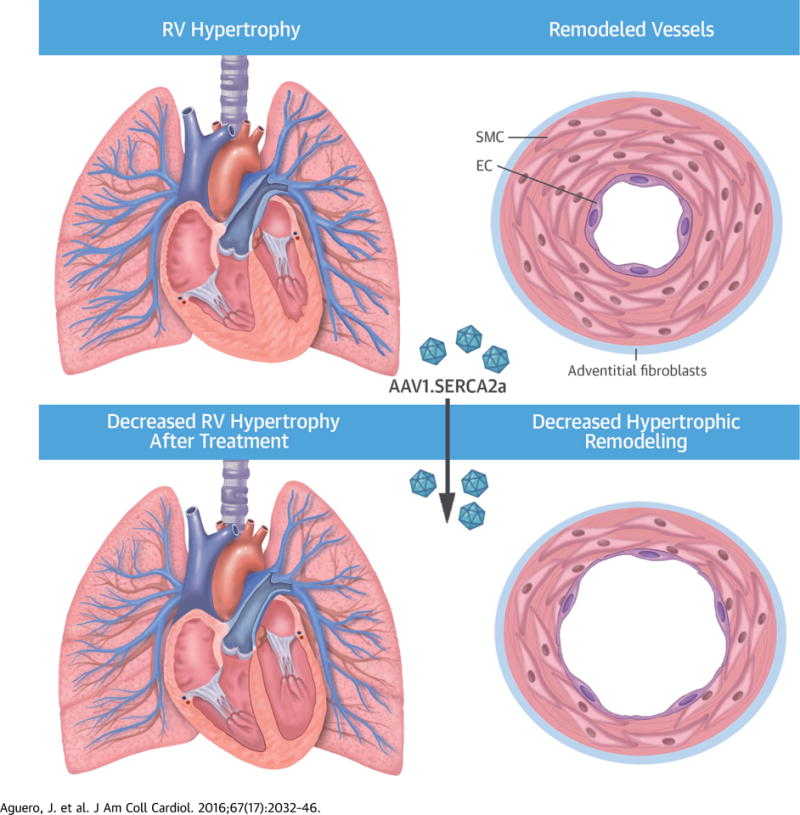
Background: Pulmonary hypertension (PH) is characterized by pulmonary arterial remodeling that results in increased pulmonary vascular resistance, right ventricular (RV) failure, and premature death. Down-regulation of sarcoplasmic reticulum Ca(2+)-ATPase 2a (SERCA2a) in the pulmonary vasculature leads to perturbations in calcium ion (Ca(2+)) homeostasis and transition of pulmonary artery smooth muscle cells to a proliferative phenotype.
Objectives: We assessed the feasibility of sustained pulmonary vascular SERCA2a gene expression using aerosolized delivery of adeno-associated virus type 1 (AAV1) in a large animal model of chronic PH and evaluated the efficacy of gene transfer regarding progression of pulmonary vascular and RV remodeling.
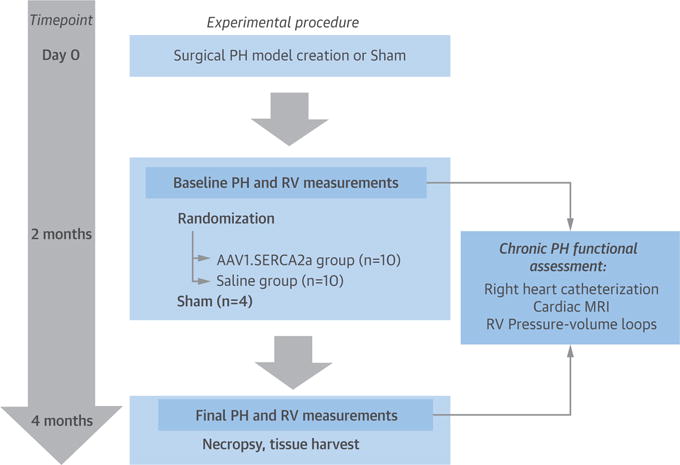
Methods: A model of chronic post-capillary PH was created in Yorkshire swine by partial pulmonary vein banding. Development of chronic PH was confirmed hemodynamically, and animals were randomized to intratracheal administration of aerosolized AAV1 carrying the human SERCA2a gene (n = 10, AAV1.SERCA2a group) or saline (n = 10). Therapeutic efficacy was evaluated 2 months after gene delivery.
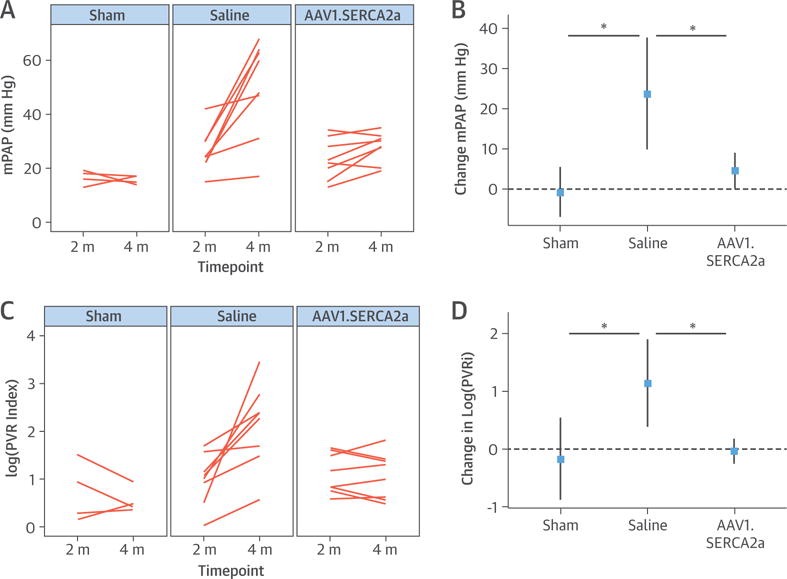
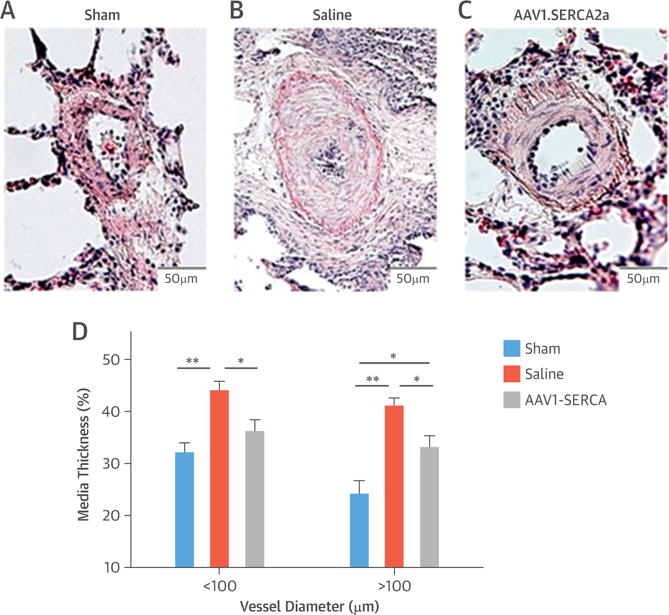
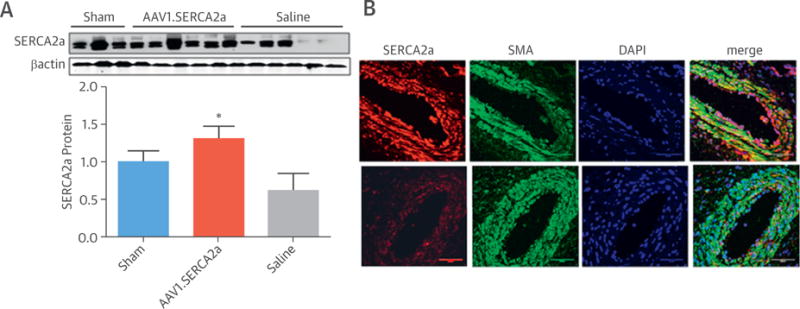
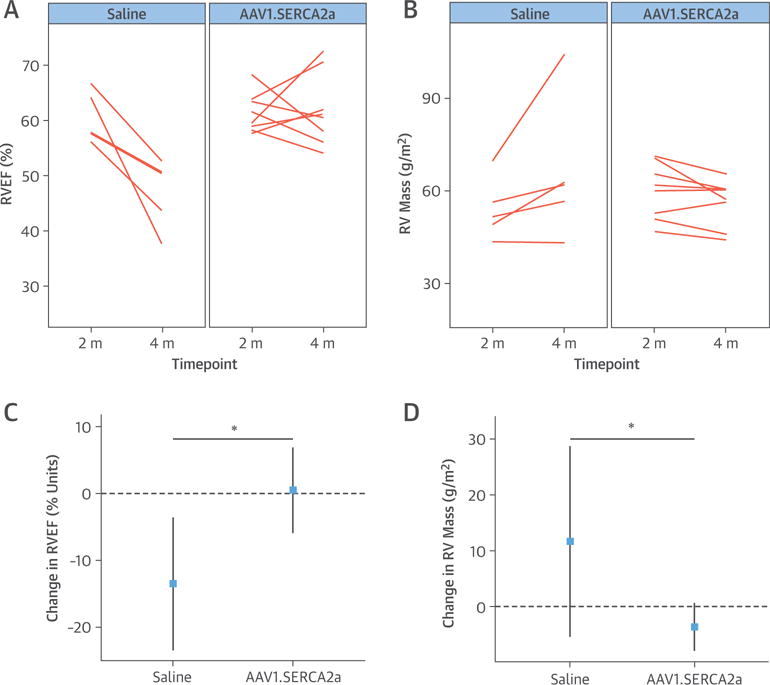
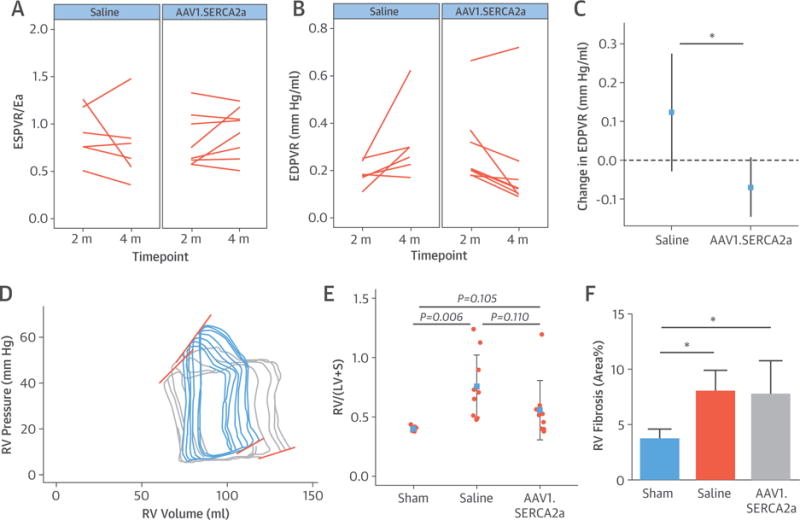
Results: Transduction efficacy after intratracheal delivery of AAV1 was confirmed by β-galactosidase detection in the distal pulmonary vasculature. Treatment with aerosolized AAV1.SERCA2a prevented disease progression as evaluated by mean pulmonary artery pressure, vascular resistance, and limited vascular remodeling quantified by histology. Therapeutic efficacy was supported further by the preservation of RV ejection fraction (p = 0.014) and improvement of the RV end-diastolic pressure-volume relationship in PH pigs treated with aerosolized AAV1.SERCA2a.
Conclusions: Airway-based delivery of AAV vectors to the pulmonary arteries was feasible, efficient, and safe in a clinically relevant chronic PH model. Vascular SERCA2a overexpression resulted in beneficial effects on pulmonary arterial remodeling, with attendant improvements in pulmonary hemodynamics and RV performance, and might offer therapeutic benefit by modifying fundamental pathophysiology in pulmonary vascular diseases.
Keywords: aerosol delivery; gene therapy; pig models; pulmonary vascular remodeling; right ventricular function.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Are Animal Models of Pulmonary Hypertension Relevant to the Clinical Disease?J Am Coll Cardiol. 2016 May 3;67(17):2047-9. doi: 10.1016/j.jacc.2016.03.002. J Am Coll Cardiol. 2016. PMID: 27126532 No abstract available.
References
-
- Galie N, Hoeper MM, Humbert M, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS) Eur Heart J. 2009;30:2493–537. - PubMed
-
- Benza RL, Miller DP, Gomberg-Maitland M, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL) Circulation. 2010;122:164–72. - PubMed
-
- van de Veerdonk MC, Kind T, Marcus JT, et al. Progressive right ventricular dysfunction in patients with pulmonary arterial hypertension responding to therapy. J Am Coll Cardiol. 2011;58:2511–9. - PubMed
-
- Vachiery JL, Adir Y, Barbera JA, et al. Pulmonary hypertension due to left heart diseases. J Am Coll Cardiol. 2013;62:D100–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
