

Sustainability of school-located influenza vaccination programs in Florida
- PMID: 27126875
- PMCID: PMC5802879
- DOI: 10.1016/j.vaccine.2016.04.017
Sustainability of school-located influenza vaccination programs in Florida
Abstract
Background: School-located influenza vaccination (SLIV) programs are a promising strategy for increasing vaccination coverage among schoolchildren. However, questions of economic sustainability have dampened enthusiasm for this approach in the United States. We evaluated SLIV sustainability of a health department led, county-wide SLIV program in Alachua County, Florida. Based on Alachua's outcome data, we modeled the sustainability of SLIV programs statewide using two different implementation costs and at different vaccination rates, reimbursement amount, and Vaccines for Children (VFC) coverage.
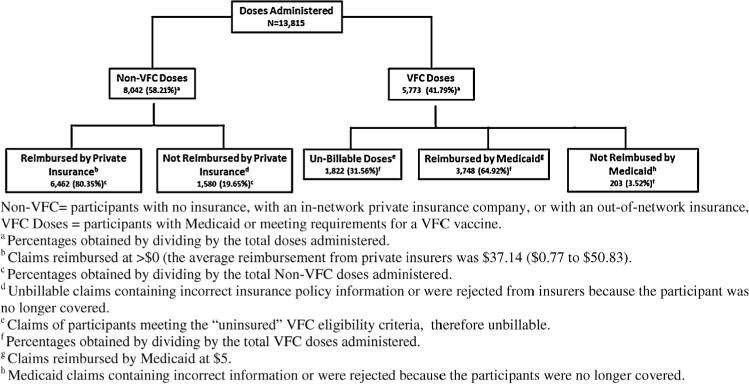
Methods: Mass vaccination clinics were conducted at 69 Alachua County schools in 2013 using VFC (for Medicaid and uninsured children) and non-VFC vaccines. Claims were processed after each clinic and submitted to insurance providers for reimbursement ($5 Medicaid and $47.04 from private insurers). We collected programmatic expenditures and volunteer hours to calculate fixed and variable costs for two different implementation costs (with or without in-kind costs included). We project program sustainability for Florida using publicly available county-specific student populations and health insurance enrollment data.
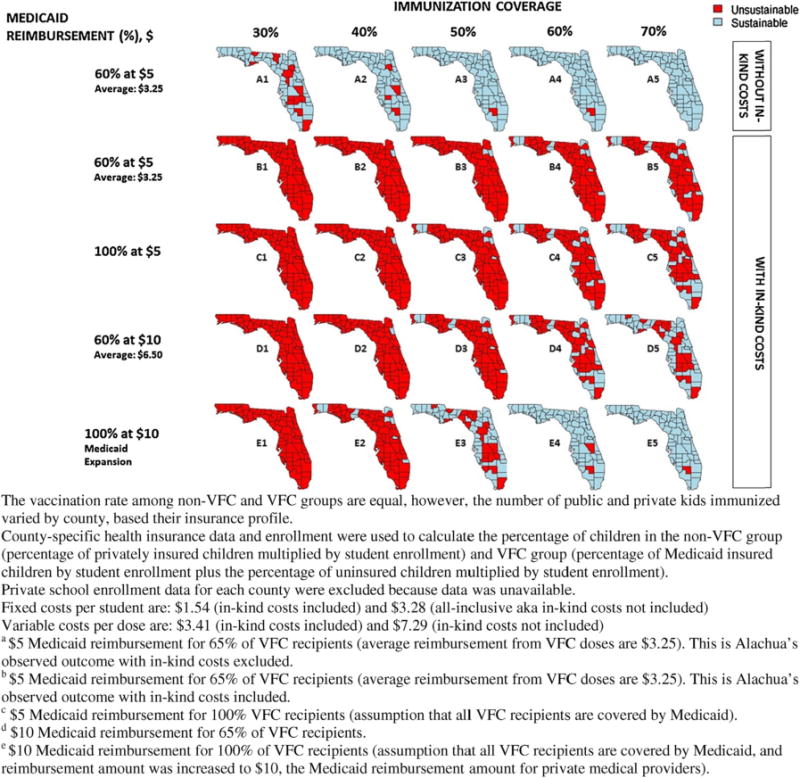
Results: Approximately 42% (n=12,853) of pre-kindergarten - 12th grade students participated in the SLIV program in Alachua. Of the 13,815 doses provided, 58% (8042) were non-VFC vaccine. Total implementation cost was $14.95/dose or $7.93/dose if "in-kind" costs were not included. The program generated a net surplus of $24,221, despite losing $4.68 on every VFC dose provided to Medicaid and uninsured children. With volunteers, 99% of Florida counties would be sustainable at a 50% vaccination rate and average reimbursement amount of $3.25 VFC and $37 non-VFC. Without volunteers, 69% of counties would be sustainable at 50% vaccination rate if all VFC recipients were on Medicaid and its reimbursement increased from $5 to $10 (amount private practices receive).
Conclusions and relevance: Key factors that contributed to the sustainability and success of an SLIV program are: targeting privately insured children and reducing administration cost through volunteers. Counties with a high proportion of VFC eligible children may not be sustainable without subsidies at $5 Medicaid reimbursement.
Keywords: Cost; Immunization; Influenza vaccination; Insurance; School health services; School-aged population.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
School-located influenza vaccination with third-party billing: outcomes, cost, and reimbursement.Acad Pediatr. 2014 May-Jun;14(3):234-40. doi: 10.1016/j.acap.2014.01.005. Acad Pediatr. 2014. PMID: 24767776 Free PMC article.
-
Cost effectiveness of school-located influenza vaccination programs for elementary and secondary school children.BMC Health Serv Res. 2019 Jun 24;19(1):407. doi: 10.1186/s12913-019-4228-5. BMC Health Serv Res. 2019. PMID: 31234842 Free PMC article. Clinical Trial.
-
Do Florida Medicaid providers' barriers to HPV vaccination vary based on VFC program participation?Matern Child Health J. 2013 May;17(4):609-15. doi: 10.1007/s10995-012-1036-5. Matern Child Health J. 2013. PMID: 22569945 Free PMC article.
-
The impact of school-located influenza vaccination programs on student absenteeism: a review of the U.S. literature.J Sch Nurs. 2011 Feb;27(1):34-42. doi: 10.1177/1059840510389182. Epub 2010 Nov 15. J Sch Nurs. 2011. PMID: 21078842 Review.
-
Current experience with school-located influenza vaccination programs in the United States: a review of the medical literature.Hum Vaccin. 2011 Feb;7(2):153-60. doi: 10.4161/hv.7.2.13668. Epub 2011 Feb 1. Hum Vaccin. 2011. PMID: 21311217 Free PMC article. Review.
Cited by
-
Influenza illness averted by influenza vaccination among school year children in Beijing, 2013-2016.Influenza Other Respir Viruses. 2018 Nov;12(6):687-694. doi: 10.1111/irv.12585. Epub 2018 Jul 1. Influenza Other Respir Viruses. 2018. PMID: 29905021 Free PMC article.
-
Behavioral determinants for vaccine acceptability among rurally located college students.Health Psychol Behav Med. 2018 Sep 6;6(1):262-276. doi: 10.1080/21642850.2018.1505519. Health Psychol Behav Med. 2018. PMID: 34040832 Free PMC article.
-
Costs of Interventions to Increase Vaccination Coverage Among Children in the United States: A Systematic Review.Acad Pediatr. 2021 May-Jun;21(4S):S67-S77. doi: 10.1016/j.acap.2020.11.015. Acad Pediatr. 2021. PMID: 33958096 Free PMC article.
-
Optimizing the impact of low-efficacy influenza vaccines.Proc Natl Acad Sci U S A. 2018 May 15;115(20):5151-5156. doi: 10.1073/pnas.1802479115. Epub 2018 Apr 30. Proc Natl Acad Sci U S A. 2018. PMID: 29712866 Free PMC article.
-
Evaluating impact of school outreach vaccination programme in Hong Kong influenza season 2018 - 2019.Hum Vaccin Immunother. 2020 Apr 2;16(4):823-826. doi: 10.1080/21645515.2019.1678357. Epub 2019 Oct 30. Hum Vaccin Immunother. 2020. PMID: 31596660 Free PMC article.
References
-
- Centers for Disease Control and Prevention. Weekly Influenza Surveillance Report Week. 2015;2 http://www.cdc.gov/flu/weekly/pdf/External_F1502.pdf [accessed January 2015.
-
- Bhat N, Wright JG, Broder KR, Murray EL, Greenberg ME, Glover MJ, et al. Influenza-associated deaths among children in the United States, 2003–2004. N Engl J Med. 2005;353:2559–67. - PubMed
-
- Influenza-associated pediatric deaths – United States, September 2010–August 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1233–8. - PubMed
-
- Fiore AE, Shay DK, Broder K, Iskander JK, Uyeki TM, Mootrey G, et al. Prevention and control of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP), 2008. MMWR Recomm Rep. 2008;57:1–60. - PubMed
-
-
Centers for Disease Control and Prevention, National Early Season Flu Vaccination Coverage, United States, November 2014.
http://www.cdc.gov/flu/fluvaxview/nifs-estimates-nov2014.htm [accessed March 2015]
-
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
