

Application of Blood-Brain Barrier Permeability Imaging in Global Cerebral Edema
- PMID: 27127002
- PMCID: PMC5018409
- DOI: 10.3174/ajnr.A4784
Application of Blood-Brain Barrier Permeability Imaging in Global Cerebral Edema
Abstract
Background and purpose: Blood-brain barrier permeability is not routinely evaluated in the clinical setting. Global cerebral edema occurs after SAH and is associated with BBB disruption. Detection of global cerebral edema using current imaging techniques is challenging. Our purpose was to apply blood-brain barrier permeability imaging in patients with global cerebral edema by using extended CT perfusion.
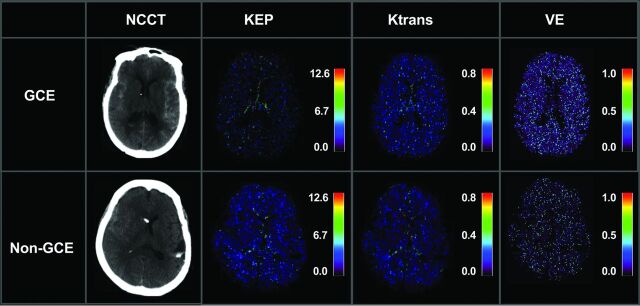
Materials and methods: Patients with SAH underwent CTP in the early phase after aneurysmal rupture (days 0-3) and were classified as having global cerebral edema or nonglobal cerebral edema using established noncontrast CT criteria. CTP data were postprocessed into blood-brain barrier permeability quantitative maps of PS (permeability surface-area product), K(trans) (volume transfer constant from blood plasma to extravascular extracellular space), Kep (washout rate constant of the contrast agent from extravascular extracellular space to intravascular space), VE (extravascular extracellular space volume per unit of tissue volume), VP (plasmatic volume per unit of tissue volume), and F (plasma flow) by using Olea Sphere software. Mean values were compared using t tests.
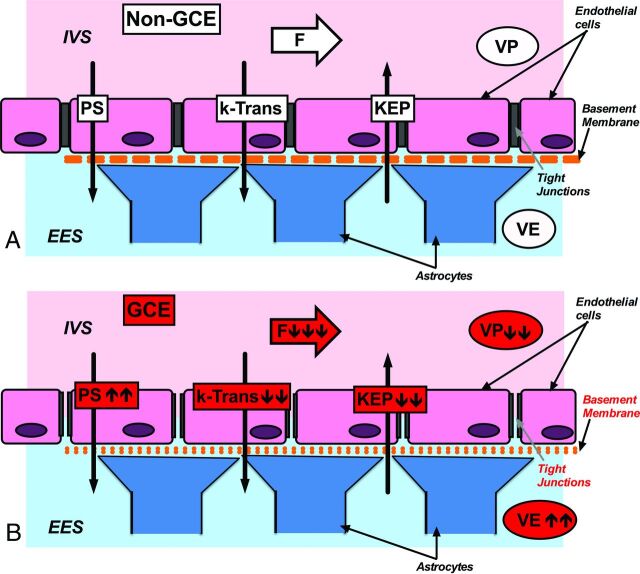
Results: Twenty-two patients were included in the analysis. Kep (1.32 versus 1.52, P < .0001), K(trans) (0.15 versus 0.19, P < .0001), VP (0.51 versus 0.57, P = .0007), and F (1176 versus 1329, P = .0001) were decreased in global cerebral edema compared with nonglobal cerebral edema while VE (0.81 versus 0.39, P < .0001) was increased.
Conclusions: Extended CTP was used to evaluate blood-brain barrier permeability in patients with SAH with and without global cerebral edema. Kep is an important indicator of altered blood-brain barrier permeability in patients with decreased blood flow, as Kep is flow-independent. Further study of blood-brain barrier permeability is needed to improve diagnosis and monitoring of global cerebral edema.
© 2016 by American Journal of Neuroradiology.
Figures
Similar articles
-
Blood-Brain Barrier Permeability in Aneurysmal Subarachnoid Hemorrhage: Correlation With Clinical Outcomes.AJR Am J Roentgenol. 2018 Oct;211(4):891-895. doi: 10.2214/AJR.17.18237. Epub 2018 Aug 7. AJR Am J Roentgenol. 2018. PMID: 30085836
-
Quantitative assessment on blood-brain barrier permeability of acute spontaneous intracerebral hemorrhage in basal ganglia: a CT perfusion study.Neuroradiology. 2017 Jul;59(7):677-684. doi: 10.1007/s00234-017-1852-9. Epub 2017 Jun 3. Neuroradiology. 2017. PMID: 28580533
-
Evaluating CT Perfusion Deficits in Global Cerebral Edema after Aneurysmal Subarachnoid Hemorrhage.AJNR Am J Neuroradiol. 2015 Aug;36(8):1431-5. doi: 10.3174/ajnr.A4328. Epub 2015 May 14. AJNR Am J Neuroradiol. 2015. PMID: 25977478 Free PMC article.
-
Potential mechanisms and clinical significance of global cerebral edema following aneurysmal subarachnoid hemorrhage.Neurosurg Focus. 2007 May 15;22(5):E7. doi: 10.3171/foc.2007.22.5.8. Neurosurg Focus. 2007. PMID: 17613238 Review.
-
Underlying Mechanisms and Potential Therapeutic Molecular Targets in Blood-Brain Barrier Disruption after Subarachnoid Hemorrhage.Curr Neuropharmacol. 2020;18(12):1168-1179. doi: 10.2174/1570159X18666200106154203. Curr Neuropharmacol. 2020. PMID: 31903882 Free PMC article. Review.
Cited by
-
CNS Drug Delivery in Stroke: Improving Therapeutic Translation From the Bench to the Bedside.Stroke. 2024 Jan;55(1):190-202. doi: 10.1161/STROKEAHA.123.043764. Epub 2023 Dec 22. Stroke. 2024. PMID: 38134249 Free PMC article. Review.
-
The Updated Role of the Blood Brain Barrier in Subarachnoid Hemorrhage: From Basic and Clinical Studies.Curr Neuropharmacol. 2020;18(12):1266-1278. doi: 10.2174/1570159X18666200914161231. Curr Neuropharmacol. 2020. PMID: 32928088 Free PMC article.
-
Alterations in Blood-Brain Barrier Permeability in Patients with Systemic Lupus Erythematosus.AJNR Am J Neuroradiol. 2019 Mar;40(3):470-477. doi: 10.3174/ajnr.A5990. Epub 2019 Feb 21. AJNR Am J Neuroradiol. 2019. PMID: 30792254 Free PMC article.
-
Hirudin Alleviates Early Brain Injury After Subarachnoid Hemorrhage in Rats via Regulating NLRP3 Inflammasome-Mediated Pyroptosis.Physiol Res. 2025 Apr 30;74(2):301-312. doi: 10.33549/physiolres.935454. Physiol Res. 2025. PMID: 40432444 Free PMC article.
-
Radiology- and gene-based risk stratification in small renal cell carcinoma: A preliminary study.PLoS One. 2021 Sep 7;16(9):e0256471. doi: 10.1371/journal.pone.0256471. eCollection 2021. PLoS One. 2021. PMID: 34492075 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources