

A randomized, comparative, open-label study of efficacy and tolerability of alfuzosin, tamsulosin and silodosin in benign prostatic hyperplasia
- PMID: 27127315
- PMCID: PMC4825428
- DOI: 10.4103/0253-7613.178825
A randomized, comparative, open-label study of efficacy and tolerability of alfuzosin, tamsulosin and silodosin in benign prostatic hyperplasia
Abstract
Objectives: Benign prostatic hyperplasia (BPH) is a common and progressive disease affecting elderly males, often associated with lower urinary tract symptoms (LUTS). α1-blockers are the mainstay in symptomatic therapy of BPH. Because of their greater uroselectivity and minimal hemodynamic effects, alfuzosin, tamsulosin, and silodosin are generally preferred. The aim of this study was to compare the efficacy and tolerability of alfuzosin, tamsulosin, and silodosin in patients with BPH and LUTS.
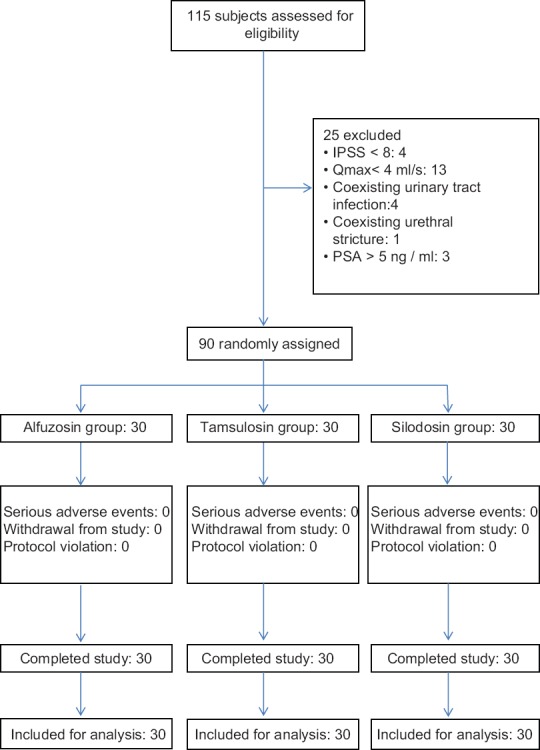
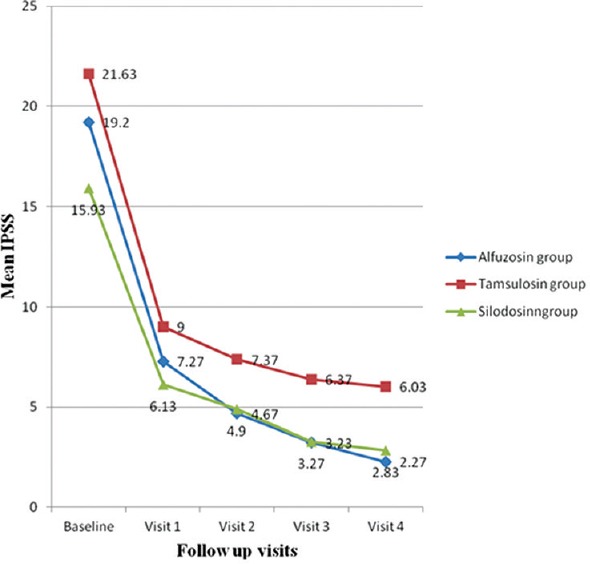
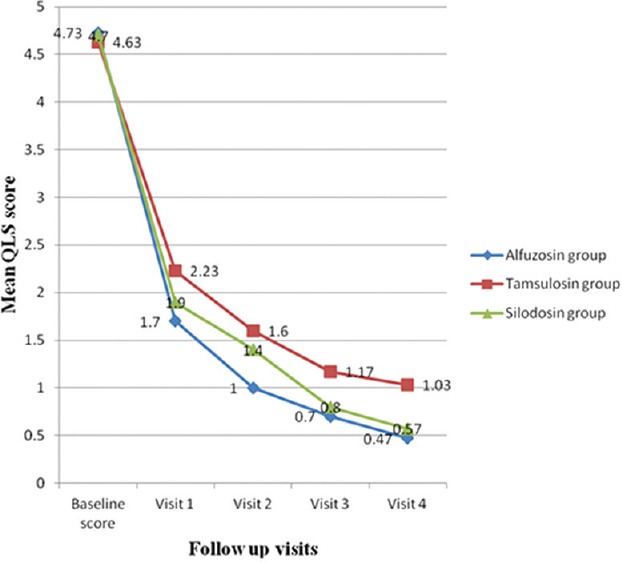
Methods: Ninety subjects with BPH and LUTS were randomized into three groups of thirty in each, to receive alfuzosin sustained release (SR) 10 mg, tamsulosin 0.4 mg, or silodosin 8 mg for 12 weeks. The primary outcome measure was a change in the International Prostate Symptom Score (IPSS), and the secondary outcome measures were changes in individual subjective symptom scores, quality of life score (QLS), and peak flow rate (Qmax) from baseline. The treatment response was monitored at 2, 4, 8, and 12 weeks.
Results: IPSS improved by 88.18%, 72.12%, and 82.23% in alfuzosin SR, tamsulosin and silodosin groups (P < 0.001) at 12 weeks. Improvement in QLS was >75% in all the three groups (P < 0.001). A significant improvement in Qmax was seen with alfuzosin and tamsulosin (P = 0.025 and P < 0.001) but not with silodosin (P = 0.153). However, the intergroup differences in IPSS, QLS, and Qmax were not significant. Ejaculatory dysfunction was more common with silodosin and corrected QT (QTc) prolongation occurred only with alfuzosin (two subjects) and tamsulosin (three subjects).
Conclusion: Alfuzosin, tamsulosin, and silodosin showed similar efficacy in improvement of LUTS secondary to BPH, with good tolerability, acceptability, and minimum hemodynamic adverse effects. Alfuzosin, tamsulosin, and silodosin are comparable in efficacy in symptomatic management of BPH. The occurrence of QTc prolongation in three subjects with tamsulosin in the present study is an unexpected adverse event as there are no reports of QTc prolongation with tamsulosin in any of the previous studies.
Keywords: alfuzosin; benign prostatic hyperplasia; clinical trial; silodosin; tamsulosin; α1-blockers.
Figures

References
-
- Rossi M, Roumeguère T. Silodosin in the treatment of benign prostatic hyperplasia. [Last cited on 2013 Mar 01];Drug Des Devel Ther. 2010 4:291–7. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2990389/ - PMC - PubMed
-
- McNicholas TA, Kirby RS, Lepor H. Evaluation and nonsurgical management of benign prostatic hyperplasia. In: Wein AJ, Kavoussi LR, Partin AW, Novick AC, Peters CA, editors. Campbell-walsh Urology. 10th ed. Philadelphia, PA: Saunders; 2012. pp. 2611–54.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
