

Coronary Stent Artifact Reduction with an Edge-Enhancing Reconstruction Kernel - A Prospective Cross-Sectional Study with 256-Slice CT
- PMID: 27128507
- PMCID: PMC4851391
- DOI: 10.1371/journal.pone.0154292
Coronary Stent Artifact Reduction with an Edge-Enhancing Reconstruction Kernel - A Prospective Cross-Sectional Study with 256-Slice CT
Abstract
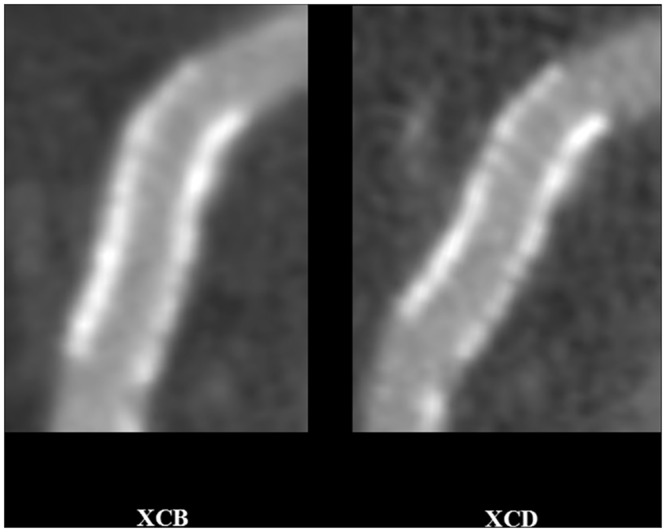
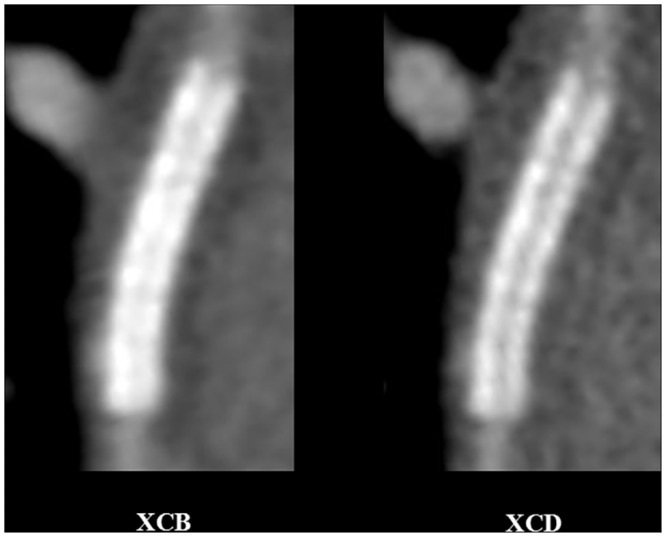
Purpose: Metallic artifacts can result in an artificial thickening of the coronary stent wall which can significantly impair computed tomography (CT) imaging in patients with coronary stents. The objective of this study is to assess in vivo visualization of coronary stent wall and lumen with an edge-enhancing CT reconstruction kernel, as compared to a standard kernel.
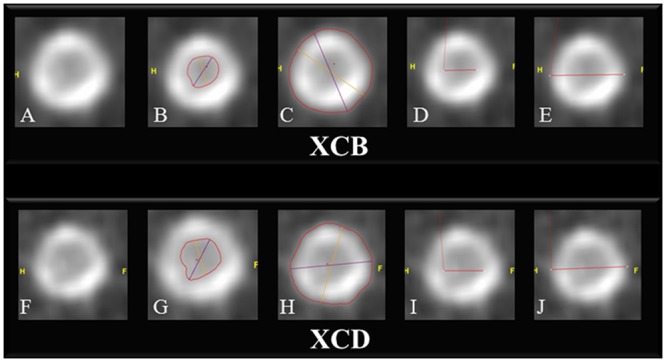
Methods: This is a prospective cross-sectional study involving the assessment of 71 coronary stents (24 patients), with blinded observers. After 256-slice CT angiography, image reconstruction was done with medium-smooth and edge-enhancing kernels. Stent wall thickness was measured with both orthogonal and circumference methods, averaging thickness from diameter and circumference measurements, respectively. Image quality was assessed quantitatively using objective parameters (noise, signal to noise (SNR) and contrast to noise (CNR) ratios), as well as visually using a 5-point Likert scale.
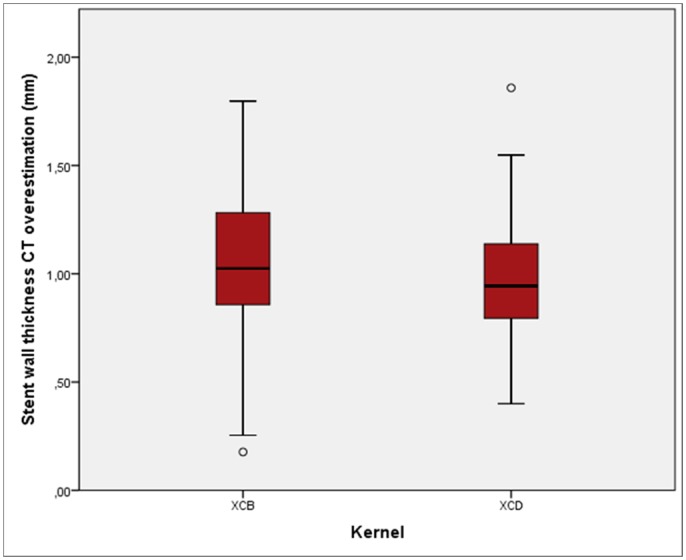
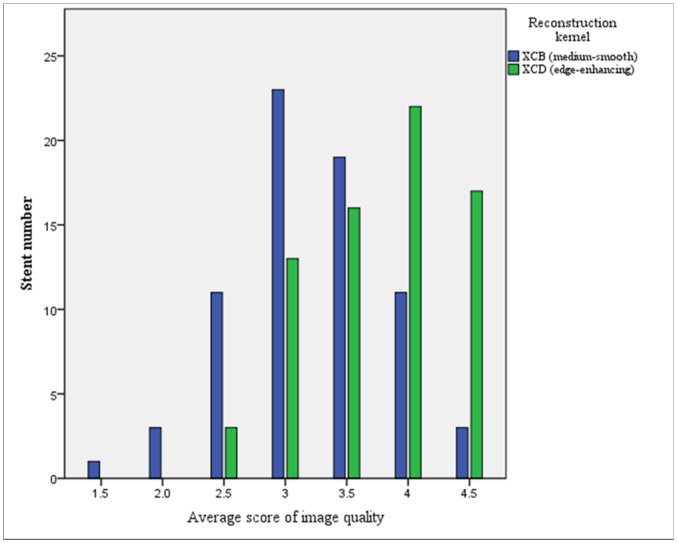
Results: Stent wall thickness was decreased with the edge-enhancing kernel in comparison to the standard kernel, either with the orthogonal (0.97 ± 0.02 versus 1.09 ± 0.03 mm, respectively; p<0.001) or the circumference method (1.13 ± 0.02 versus 1.21 ± 0.02 mm, respectively; p = 0.001). The edge-enhancing kernel generated less overestimation from nominal thickness compared to the standard kernel, both with the orthogonal (0.89 ± 0.19 versus 1.00 ± 0.26 mm, respectively; p<0.001) and the circumference (1.06 ± 0.26 versus 1.13 ± 0.31 mm, respectively; p = 0.005) methods. The edge-enhancing kernel was associated with lower SNR and CNR, as well as higher background noise (all p < 0.001), in comparison to the medium-smooth kernel. Stent visual scores were higher with the edge-enhancing kernel (p<0.001).
Conclusion: In vivo 256-slice CT assessment of coronary stents shows that the edge-enhancing CT reconstruction kernel generates thinner stent walls, less overestimation from nominal thickness, and better image quality scores than the standard kernel.
Conflict of interest statement
Figures
Similar articles
-
Computed tomography coronary stent imaging with iterative reconstruction: a trade-off study between medium kernel and sharp kernel.J Comput Assist Tomogr. 2014 Jul-Aug;38(4):604-12. doi: 10.1097/RCT.0000000000000080. J Comput Assist Tomogr. 2014. PMID: 24651753
-
Coronary stent imaging with dual-source CT: assessment of lumen visibility using different convolution kernels and postprocessing filters.Acta Radiol. 2015 Jan;56(1):42-50. doi: 10.1177/0284185113517229. Epub 2014 Jan 7. Acta Radiol. 2015. PMID: 24399513
-
Photon Counting Computed Tomography With Dedicated Sharp Convolution Kernels: Tapping the Potential of a New Technology for Stent Imaging.Invest Radiol. 2018 Aug;53(8):486-494. doi: 10.1097/RLI.0000000000000485. Invest Radiol. 2018. PMID: 29794949
-
Assessment of coronary artery stents using 16-slice MDCT angiography: evaluation of a dedicated reconstruction kernel and a noise reduction filter.Eur Radiol. 2005 Apr;15(4):721-6. doi: 10.1007/s00330-004-2594-8. Epub 2005 Feb 12. Eur Radiol. 2005. PMID: 15711845
-
Coronary Stent Imaging with Photon-counting Detector CT.Radiol Cardiothorac Imaging. 2025 Jun;7(3):e240338. doi: 10.1148/ryct.240338. Radiol Cardiothorac Imaging. 2025. PMID: 40439564 Review.
Cited by
-
Stent evaluation by coronary computed tomography angiography: a comparison between Iopamidol-370 and Ioversol-320 hypo-osmolar iodine concentration contrasts.Br J Radiol. 2020 Nov 1;93(1115):20200078. doi: 10.1259/bjr.20200078. Epub 2020 Aug 20. Br J Radiol. 2020. PMID: 32816561 Free PMC article. Clinical Trial.
-
Computed tomography in paediatric heart disease.Br J Radiol. 2018 Dec;91(1092):20180201. doi: 10.1259/bjr.20180201. Epub 2018 Aug 13. Br J Radiol. 2018. PMID: 30004804 Free PMC article. Review.
-
Comparison of different CT metal artifact reduction strategies for standard titanium and carbon-fiber reinforced polymer implants in sheep cadavers.BMC Med Imaging. 2021 Feb 15;21(1):29. doi: 10.1186/s12880-021-00554-y. BMC Med Imaging. 2021. PMID: 33588781 Free PMC article.
-
Effectiveness of wedge filter application in reducing lens radiation dose during diagnostic cerebral angiography: a phantom and prospective study.Eur Radiol. 2025 Oct;35(10):5996-6004. doi: 10.1007/s00330-025-11617-x. Epub 2025 Apr 26. Eur Radiol. 2025. PMID: 40285813
-
Dual-energy CT and ceramic or titanium prostheses material reduce CT artifacts and provide superior image quality of total knee arthroplasty.Knee Surg Sports Traumatol Arthrosc. 2019 May;27(5):1552-1561. doi: 10.1007/s00167-018-5001-8. Epub 2018 Jun 7. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 29881885 Free PMC article.
References
-
- Kruger S, Mahnken AH, Sinha AM, Borghans A, Dedden K, Hoffmann R, et al. Multislice spiral computed tomography for the detection of coronary stent restenosis and patency. Int J Cardiol. 2003; 89:167–172. - PubMed
-
- Cademartiri F, Schuijf JD, Pugliese F, Mollet NR, Jukema JW, Maffei E, et al. Usefulness of 64-slice multislice computed tomography coronary angiography to assess in-stent restenosis. J Am Coll Cardiol. 2007; 49:2204–2210. - PubMed
-
- Seifarth H, Ozgun M, Raupach R, Flohr T, Heindel W, Fischbach R et al. 64- versus 16-slice CT angiography for coronary artery stent assessment: In vitro experience. Invest Radiol. 2006; 41:22–27. - PubMed
-
- Pugliese F, Weustink AC, Van Mieghem C, Alberghina F, Otsuka M, Meijboom WB, et al. Dual source coronary computed tomography angiography for detecting in-stent restenosis. Heart. 2008. 94:848–854. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
