

Epidemiology and trends in non-fatal self-harm in three centres in England, 2000-2012: findings from the Multicentre Study of Self-harm in England
- PMID: 27130163
- PMCID: PMC4854013
- DOI: 10.1136/bmjopen-2015-010538
Epidemiology and trends in non-fatal self-harm in three centres in England, 2000-2012: findings from the Multicentre Study of Self-harm in England
Abstract
Objectives: Self-harm is a major health problem in many countries, with potential adverse outcomes including suicide and other causes of premature death. It is important to monitor national trends in this behaviour. We examined trends in non-fatal self-harm and its management in England during the 13-year period, 2000-2012.
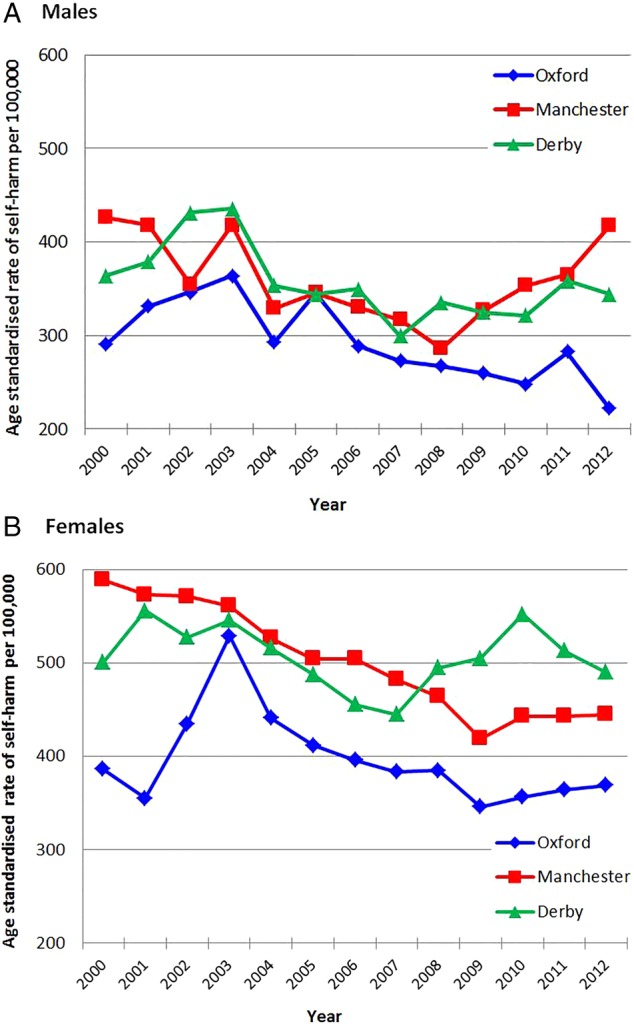
Design and setting: This observational study was undertaken in the three centres of the Multicentre Study of Self-harm in England. Information on all episodes of self-harm by individuals aged 15 years and over presenting to five general hospitals in three cities (Oxford, Manchester and Derby) was collected through face-to-face assessment or scrutiny of emergency department electronic databases. We used negative binomial regression models to assess trends in rates of self-harm and logistic regression models for binary outcomes (eg, assessed vs non-assessed patients).
Participants: During 2000-2012, there were 84,378 self-harm episodes (58.6% by females), involving 47,048 persons.
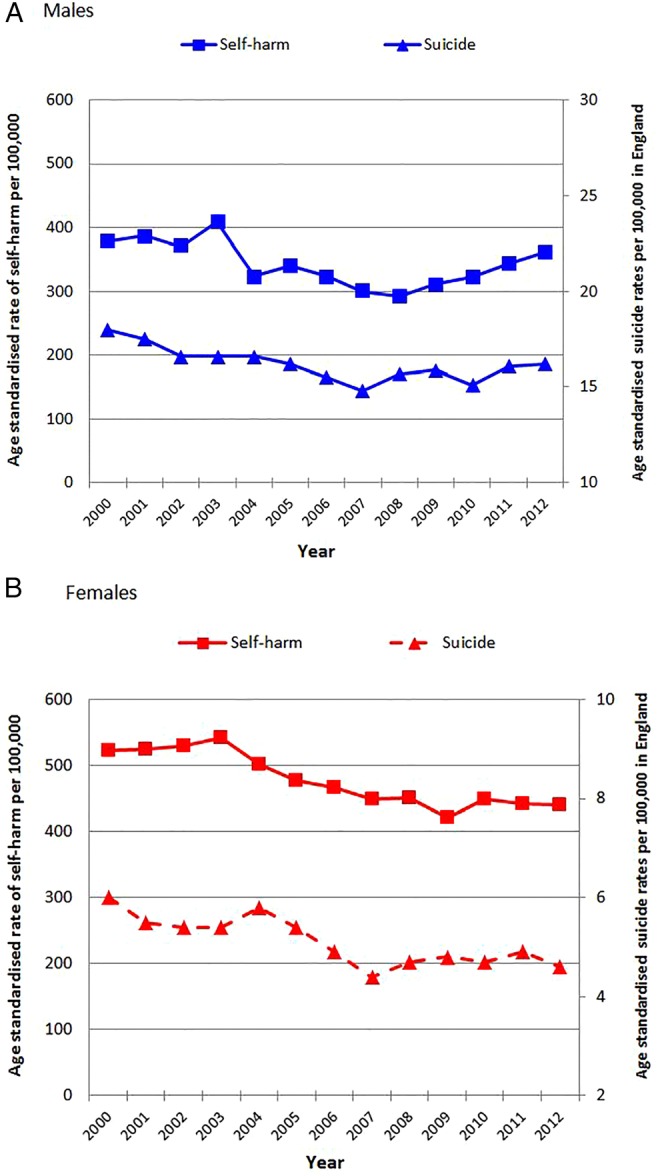
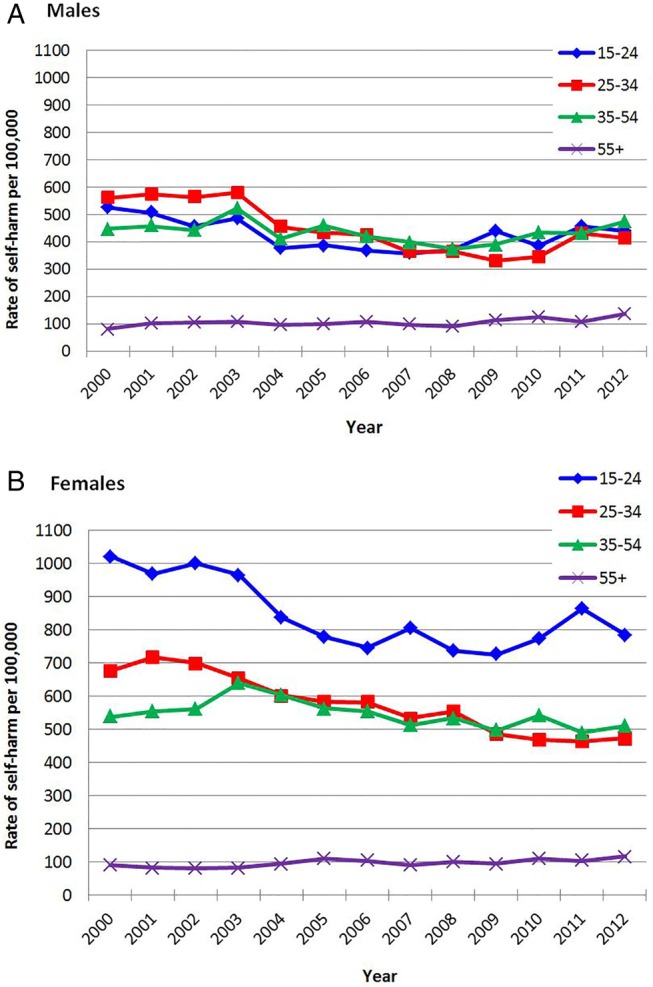
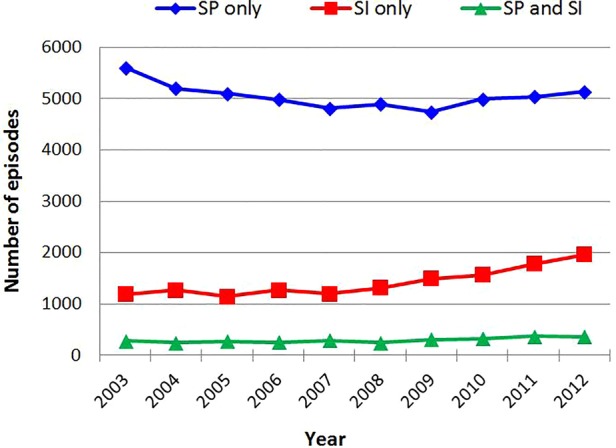
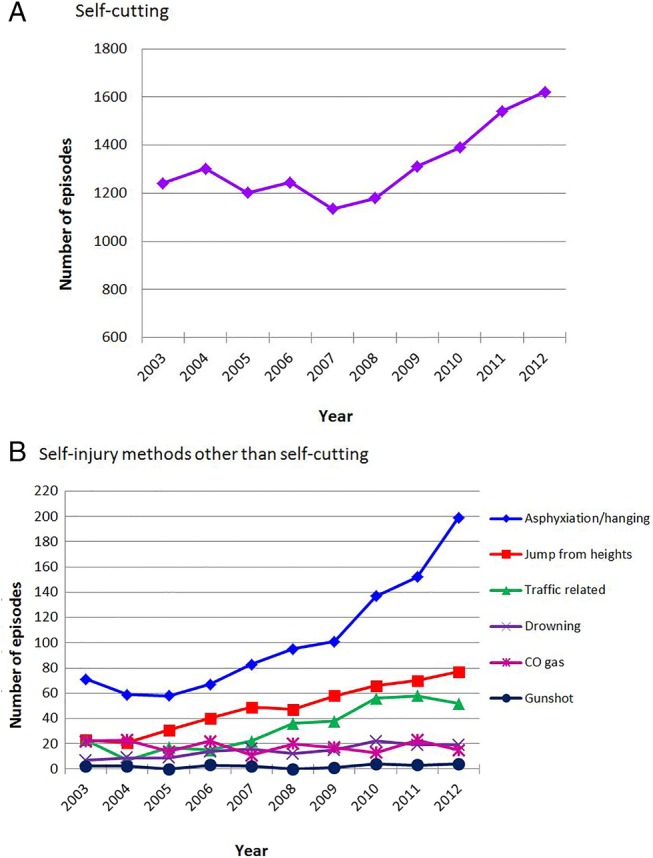
Results: Rates of self-harm declined in females (incidence rate ratio (IRR) 0.98; 95% CI 0.97 to 0.99, p<0.0001). In males, rates of self-harm declined until 2008 (IRR 0.96; 95% CI 0.95 to 0.98, p<0.0001) and then increased (IRR 1.05; 95% CI 1.02 to 1.09, p=0.002). Rates of self-harm were strongly correlated with suicide rates in England in males (r=0.82, p=0.0006) and females (r=0.74, p=0.004). Over 75% of self-harm episodes were due to self-poisoning, mainly with analgesics (45.7%), antidepressants (24.7%) and benzodiazepines (13.8%). A substantial increase in self-injury occurred in the latter part of the study period. This was especially marked for self-cutting/stabbing and hanging/asphyxiation. Psychosocial assessment by specialist mental health staff occurred in 53.2% of episodes.
Conclusions: Trends in rates of self-harm and suicide may be closely related; therefore, self-harm can be a useful mental health indicator. Despite national guidance, many patients still do not receive psychosocial assessment, especially those who self-injure.
Keywords: EPIDEMIOLOGY; PUBLIC HEALTH.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical