

Unconventional Volume-Outcome Associations in Adult Extracorporeal Membrane Oxygenation in the United States
- PMID: 27130248
- PMCID: PMC5835397
- DOI: 10.1016/j.athoracsur.2016.02.009
Unconventional Volume-Outcome Associations in Adult Extracorporeal Membrane Oxygenation in the United States
Abstract
Background: The aim of this study was to evaluate institutional volume-outcome relationships in extracorporeal membrane oxygenation (ECMO) with subanalyses of ECMO in patients with a primary diagnosis of respiratory failure.
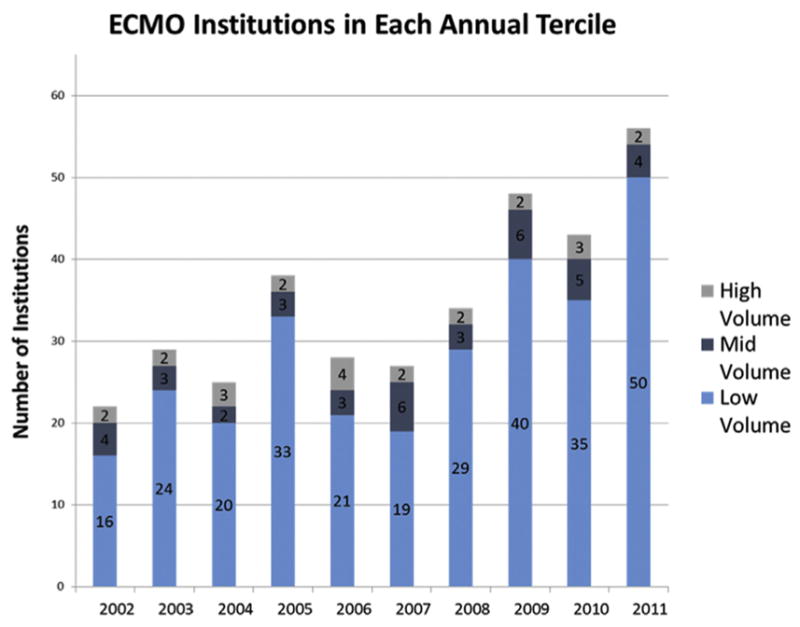
Methods: All institutions with adult ECMO discharges in the Nationwide Inpatient Sample from 2002 to 2011 were evaluated. International Classification of Diseases (ninth revision) codes were used to identify ECMO-treated patients, indications, and concurrent procedures. Patients who were treated with ECMO after cardiotomy were excluded. Annual institutional and national volume of ECMO hospitalizations varied widely, hence the number of ECMO cases performed at an institution was calculated for each year independently. Institutions were grouped into high-, medium-, and low-volume terciles by year. Statistical analysis included hierarchical, multivariable logistic regression.
Results: The in-hospital mortality rates for ECMO admissions at low-, medium-, and high-volume ECMO centers were 48% (n = 467), 60% (n = 285), and 57% (n = 445), respectively (p = 0.001). In post hoc pairwise comparisons, patients in low-volume hospitals were more likely to survive to discharge compared with patients in medium-volume (p = 0.001) and high-volume (p = 0.005) hospitals. There was no significant difference in survival between medium-volume and high-volume hospitals (p = 0.81). In a subanalysis of patients with respiratory failure, low-volume ECMO centers maintained the lowest rates of in-hospital mortality (47%), versus 61% in medium-volume institutions (p = 0.045) and 56% in high-volume institutions (p = 0.15). Multivariable logistical regression produced similar results in the entire study sample and in patients with respiratory failure.
Conclusions: ECMO outcomes in the Nationwide Inpatient Sample do not follow a traditional volume-outcome relationship, and these results suggest that, in properly selected patients, ECMO can be performed with acceptable results in U.S. centers that do not perform a high volume of ECMO.
Copyright © 2016 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Hill JD, O’Brien TG, Murray JJ, et al. Prolonged extracorporeal oxygenation for acute post-traumatic respiratory failure (shock-lung syndrome) use of the Bramson membrane lung. N Engl J Med. 1972;286:629–34. - PubMed
-
- Zapol WM, Snider MT, Hill J, et al. Extracorporeal membrane oxygenation in severe acute respiratory failure: a randomized prospective study. JAMA. 1979;242:2193–6. - PubMed
-
- McCarthy FH, McDermott KM, Kini V, et al. Trends in U.S. extracorporeal membrane oxygenation utilization and outcomes: 2002–2012. Paper presented at 95th annual meeting of the American Association for Thoracic Surgery; April 25–29, 2015; Seattle, WA.
-
- Peek GJ, Mugford M, Tiruvoipati R, et al. Efficacy and Economic Assessment of Conventional Ventilatory Support Versus Extracorporeal Membrane Oxygenation for Severe Adult Respiratory Failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009;374:1351–63. - PubMed
-
- Sidebotham D, McGeorge A, McGuinness S, Edwards M, Willcox T, Beca J. Extracorporeal membrane oxygenation for treating severe cardiac and respiratory disease in adults. Part 1: overview of extracorporeal membrane oxygenation. J Cardiothorac Vasc Anesth. 2009;23:886–92. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
