

Dual-mobility or Constrained Liners Are More Effective Than Preoperative Bariatric Surgery in Prevention of THA Dislocation
- PMID: 27130648
- PMCID: PMC5014805
- DOI: 10.1007/s11999-016-4859-3
Dual-mobility or Constrained Liners Are More Effective Than Preoperative Bariatric Surgery in Prevention of THA Dislocation
Abstract
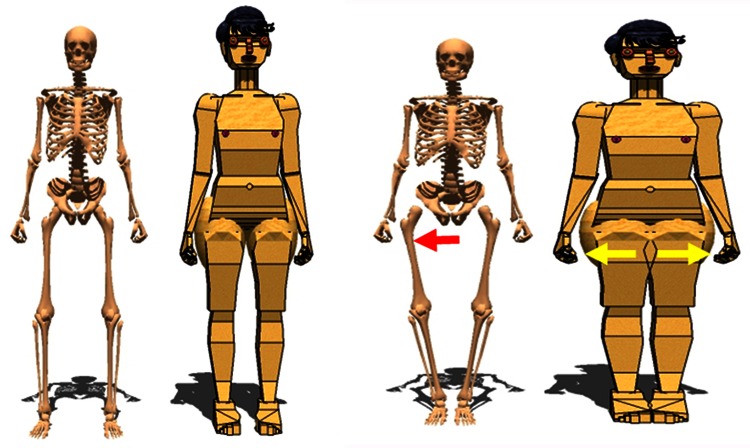
Background: Obesity is associated with an increased risk of dislocation after total hip arthroplasty (THA). However, in patients with obesity, it is not known whether the risk is only in the early postoperative period or whether it persists several years after surgery, and whether having bariatric surgery before undergoing THA and/or receiving a specific device (such as a dual-mobility or constrained acetabular liner) is more effective in terms of decreasing the risk of dislocation.
Question/purposes: (1) What is the cumulative risk of dislocation in patients with obesity after THA in the absence of a dual-mobility or constrained liner, and is this related to component positioning? (2) Does bariatric surgery before undergoing THA decrease dislocation risk in patients with obesity? (3) Are dual-mobility and constrained liners efficient in preventing dislocation in patients with obesity?
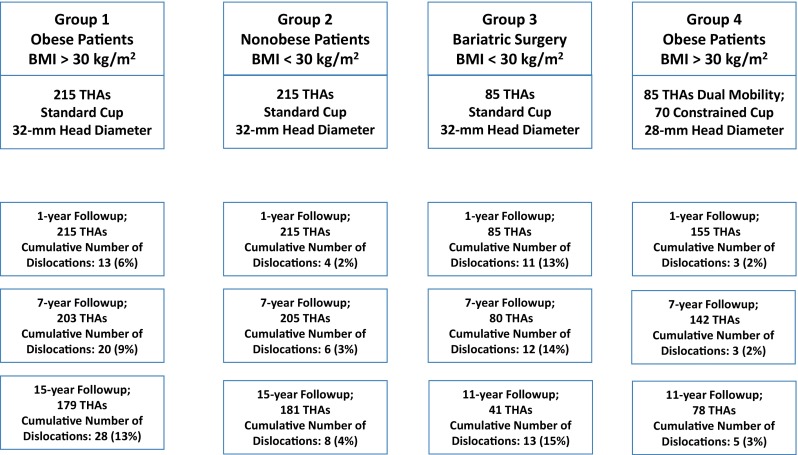
Methods: At our university-based practice, all surgeons adhered to the following treatment approaches: Before 2000 no dual-mobility implants or constrained liners were used for primary THAs. Between 2000 and 2008, all patients whose body mass index (BMI) was greater than 30 kg/m(2) received dual-mobility liners (or constrained liners), except when they had previously had bariatric surgery. After 2008, all patients with BMIs over 30 kg/m(2) as well as those patients who were previously treated with bariatric surgery (regardless of BMI at the time of the index THA) received dual-mobility or constrained liners. This case-control study compared the dislocation percentage between 215 hips in nonobese patients (BMI ≤ 30 kg/m(2)), 215 hips in patients with obesity (BMI > 30 kg/m(2)) who received standard cups, 85 hips in patients with bariatric surgery before THA using standard cups (with reduction to a BMI < 30 kg/m(2)), and 155 hips in patients with obesity who received dual-mobility (when younger than 70 years) or constrained liners (when older than 70 years). All patients received the same implants except for different femoral head diameters (32-mm head with standard cups and 28-mm head with dual-mobility or constrained liners). The patients were followed at routine intervals and were specifically queried about dislocation. All the 670 hips had a minimum followup of 5 years with a mean followup of 14 years (range 5-25 years). At the most recent followup, 101 (15%) hips were lost to followup (respectively, 36 of 215, 34 of 215, five of 85, 24 of 155), which is the same ratio as observed among the underlying populations from which the patients were drawn.
Results: With standard liners, more hips in patients with BMI > 30 kg/m(2) dislocated than did hips in nonobese (BMI < 30 kg/m(2)) patients. The cumulative number of dislocations (first time without recurrent dislocation) was 6% (13 of 215) at 1-year followup in obese patients compared with 2% (four of 215) in nonobese patients (odds ratio [OR], 3.4; 95% confidence interval [CI] 1.09-10.58; p = 0.03) and was 13% (28 of 215) at 15 years followup compared with 4% (eight of 215) in nonobese patients (OR, 3.9; 95% CI 1.72-8.71; p = 0.001). When bariatric surgery was performed before THA, BMI declined from 42 kg/m(2) to 28 kg/m(2), but with the same standard liners, more hips after bariatric surgery dislocated at 1-year followup than did hips in patients with obesity without preoperative bariatric surgery (13% [11 of 85] compared with 6% [13 of 215]; OR, 0.43; 95% CI 0.18-1.01; p = 0.05). Dual-mobility or constrained implants decreased the risk of dislocation, and fewer hips in patients with obesity with dual-mobility or constrained liners at 7 years followup had dislocated than did hips with standard liners (2% [three of 155] compared with 9% [20 of 215]; OR, 0.19; 95% CI 0.05-0.66; p = 0.01) bringing this number in line with the number observed in nonobese subjects with standard cups.
Conclusions: With standard liners, the risk of dislocation is increased in patients with obesity. Preoperative decrease of BMI (with bariatric surgery) in patients with obesity did not prevent the risk of dislocation with standard liners. Use of dual-mobility or constrained liners in these patients is an effective technique to reduce the risk of postoperative hip dislocation. However, we do not yet know the full risks of loosening of dual-mobility and constrained liners in this obese population.
Level of evidence: Level III, therapeutic study.
Figures
Comment in
-
CORR Insights(®): Dual-mobility or Constrained Liners Are More Effective Than Preoperative Bariatric Surgery in Prevention of THA Dislocation.Clin Orthop Relat Res. 2016 Oct;474(10):2211-2. doi: 10.1007/s11999-016-4901-5. Epub 2016 May 25. Clin Orthop Relat Res. 2016. PMID: 27225703 Free PMC article. No abstract available.
References
-
- Berry DJ, Von Knoch M, Schleck CD, Harmsen WS. The cumulative long-term risk of dislocation after primary Charnley total hip arthroplasty. J Bone Joint Surg Am. 2004;86:9–14. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
