

Effect of Ownership on Hospice Service Use: 2005-2011
- PMID: 27131344
- PMCID: PMC4882235
- DOI: 10.1111/jgs.14093
Effect of Ownership on Hospice Service Use: 2005-2011
Abstract
Objectives: To assess differences in populations and service use according to hospice ownership, chain status, and agency size.
Design: Retrospective cohort study.
Setting: United States.
Participants: Medicare beneficiaries aged 65 and older enrolled in hospice during 2005 to 2011 N = 5,405,526).
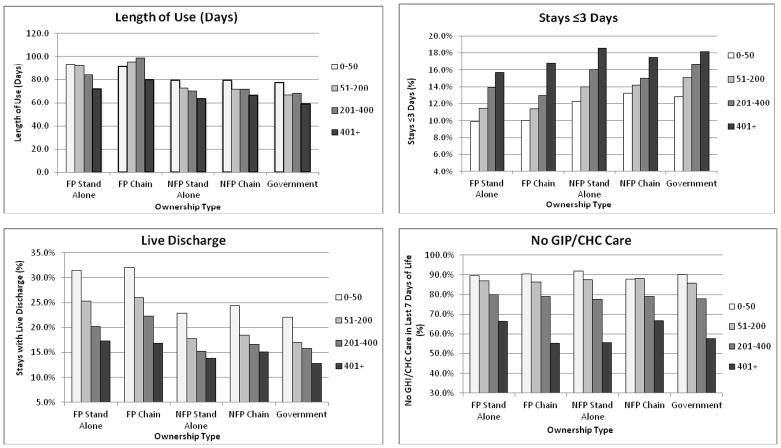
Measurements: Hospice use according to ownership category (for-profit nonchain and chain, not-for-profit nonchain and chain, government) and agency size (0-50, 51-200, 201-400, ≥401 individuals discharged each year). Mean length of use, stays of 3 days or fewer, stays ending with live discharge, and decedents receiving no general inpatient care (GIP)- or continuous home care (CHC)-level hospice in the last 7 days of life.
Results: After adjusting for individual and geographic differences, for-profit nonchain and chain agencies had longer mean length of use (84.5 and 91.2 days, respectively) than other agency types (66.3-72.5 days), higher rates of live discharge (21.0% and 20.2% vs 14.6-15.9%), and lower proportions of stays of 3 days or fewer (13.9% and 14.7% vs 16.6-17.5%) (all P < .001). The proportion of decedents not receiving GIP- or CHC-level care before death was highest in for-profit chains (75.9%) and lowest in not-for-profit nonchains (63.2%). Smaller agencies had longer mean length of use, higher live discharge rates, lower rates of stays of 3 days or fewer, and higher rates of individuals receiving no GIP- or CHC-level care. There were considerable differences in patient traits and unadjusted service use between the nation's largest chains.
Conclusion: In addition to for-profit and not-for-profit hospice agencies differing according to important dimensions, there is substantial heterogeneity within these ownership categories, highlighting the need to consider factors such as agency size and chain affiliation in understanding variations in Medicare beneficiaries' hospice care.
Keywords: Medicare; hospice; ownership; profit; quality.
© 2016, Copyright the Authors Journal compilation © 2016, The American Geriatrics Society.
Conflict of interest statement
Figures
References
-
- IOM (Institute of Medicine) Dying in America: Improving quality and honoring individual preferences near the end of life. Washington, D.C: The National Academies Press; 2014. - PubMed
-
- MedPAC. Hospice Services. Report to the Congress: Medicare Payment Policy (March 2014) Washington, D.C: The Medicare Payment Advisory Commission; 2014. pp. 299–320.
-
- Span P. The New Old Age: Caring and Coping [Internet] [Accessed October 12, 2014];New York Times. 2014 Oct 6; Available at: http://newoldage.blogs.nytimes.com/2014/10/06/extra-scrutiny-for-hospices/
-
- Lindrooth RC, Weisbrod BA. Do religious nonprofit and for-profit organizations respond differently to financial incentives? The hospice industry. J Health Econ. 2007;26:342–357. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
