

Interleukin 6 Is a Stronger Predictor of Clinical Events Than High-Sensitivity C-Reactive Protein or D-Dimer During HIV Infection
- PMID: 27132283
- PMCID: PMC4936649
- DOI: 10.1093/infdis/jiw173
Interleukin 6 Is a Stronger Predictor of Clinical Events Than High-Sensitivity C-Reactive Protein or D-Dimer During HIV Infection
Abstract
Background: Interleukin 6 (IL-6), high-sensitivity C-reactive protein (hsCRP), and D-dimer levels are linked to adverse outcomes in human immunodeficiency virus (HIV) infection, but the strength of their associations with different clinical end points warrants investigation.
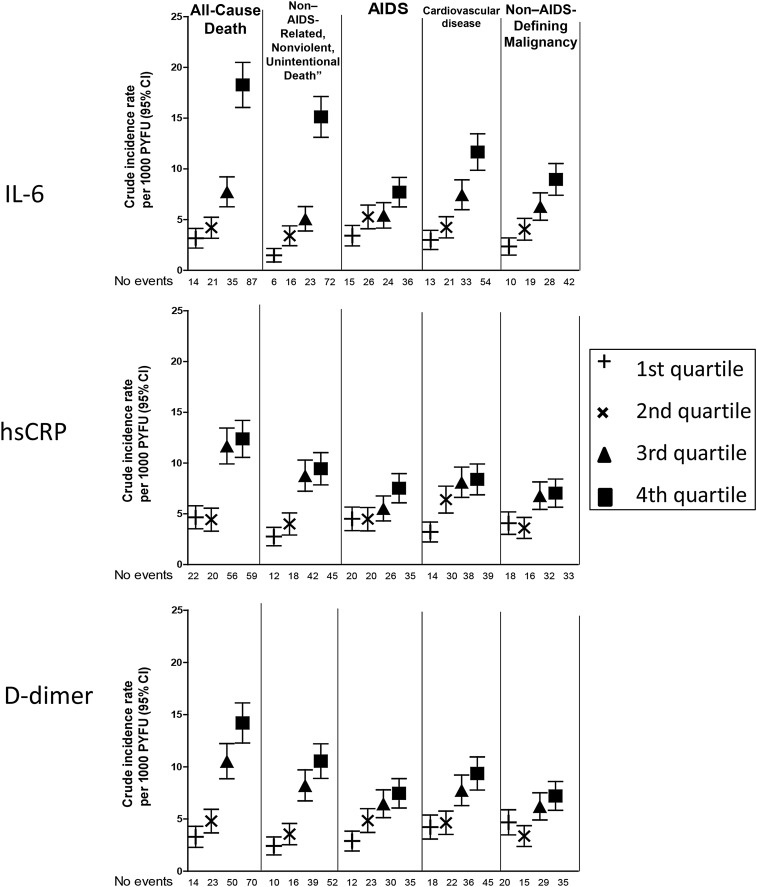
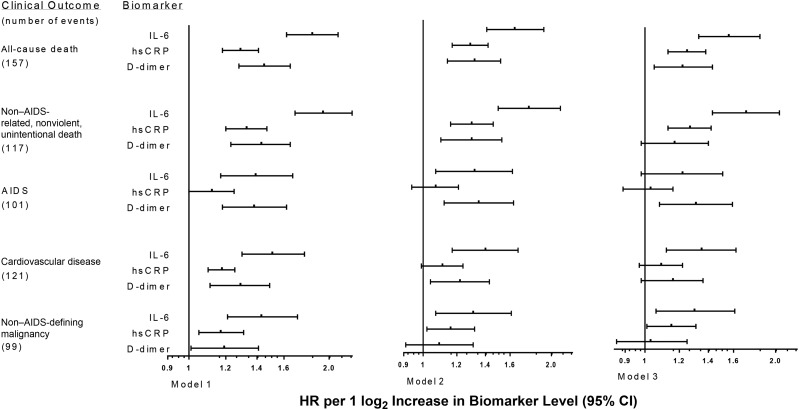
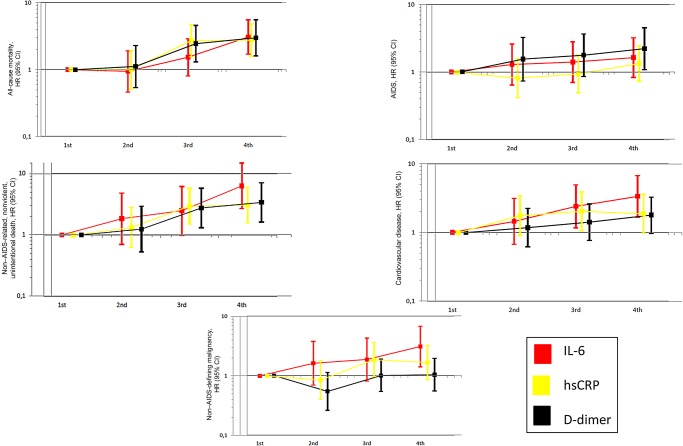
Methods: Participants receiving standard of care in 2 HIV trials with measured biomarker levels were followed to ascertain all-cause death, non-AIDS-related death, AIDS, cardiovascular disease (CVD), and non-AIDS-defining malignancies. Hazard ratios (HRs) and 95% confidence intervals (CIs) of each end point for quartiles and log2-transformed IL-6, hsCRP, and D-dimer levels were calculated using Cox models. Marginal models modelling multiple events tested for equal effects of biomarker levels on different end points.
Results: Among 4304 participants, there were 157 all-cause deaths, 117 non-AIDS-related deaths, 101 AIDS cases, 121 CVD cases, and 99 non-AIDS-defining malignancies. IL-6 was more strongly associated with most end points, compared with hsCRP. IL-6 appeared to be a stronger predictor than D-dimer for CVD and non-AIDS-defining malignancies, but 95% CIs overlapped. Independent associations of IL-6 were stronger for non-AIDS-related death (HR, 1.71; 95% CI, 1.43-2.04) and all-cause death (HR, 1.56; 95% CI, 1.33-1.84) and similar for CVD (HR, 1.35; 95% CI, 1.12-1.62) and non-AIDS-defining malignancies (HR, 1.30; 95% CI, 1.06-1.61). There was heterogeneity of IL-6 (P < .001) but not hsCRP (P = .15) or D-dimer (P = .20) as a predictor for different end points.
Conclusions: IL-6 is a stronger predictor of fatal events than of CVD and non-AIDS-defining malignancies. Adjuvant antiinflammatory and antithrombotic therapies should be tested in HIV-infected individuals.
Keywords: D-dimer; HIV; IL-6; cancer; cardiovascular disease; hsCRP; inflammation.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail journals.permissions@oup.com.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
