

Impact of Weight Loss Surgery on Esophageal Physiology
- PMID: 27134597
- PMCID: PMC4849509
Impact of Weight Loss Surgery on Esophageal Physiology
Abstract
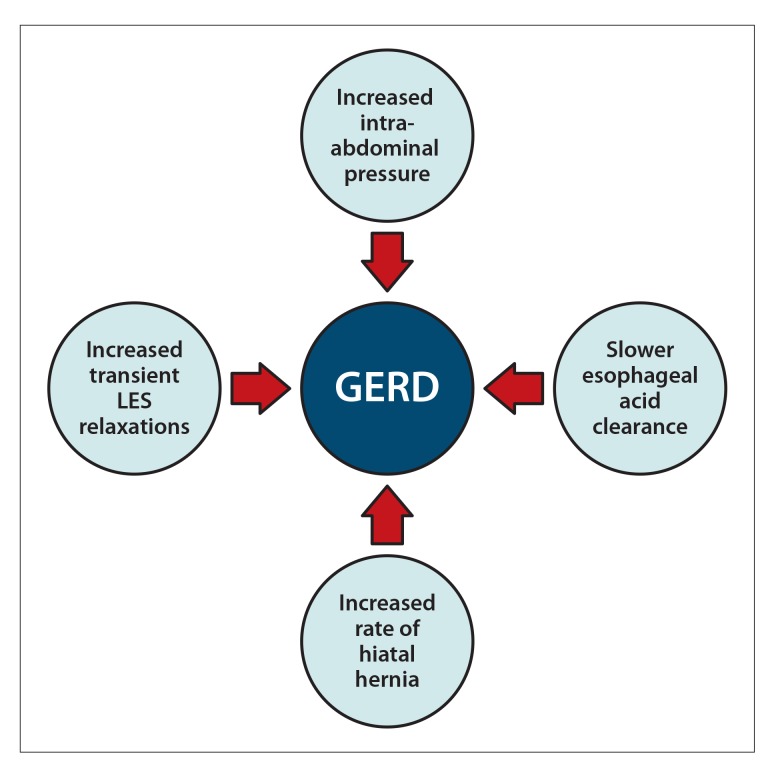
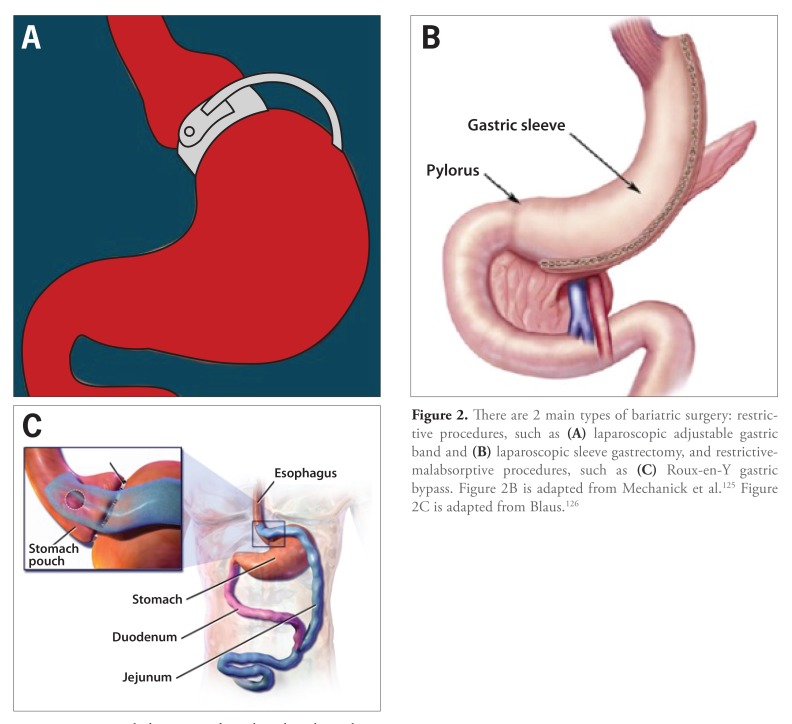
Bariatric surgery has come to the forefront of weight loss treatment due to its complex interactions via anatomic, physiologic, and neurohormonal changes leading to sustained weight loss. Unlike lifestyle and pharmacologic options, which fail to show long-term sustained weight loss, bariatric surgery has been shown to decrease overall mortality and morbidity. Bariatric surgery can be purely restrictive, such as laparoscopic adjustable gastric band (LAGB) or laparoscopic sleeve gastrectomy (LSG), or restrictive-malabsorptive, such as Roux-en-Y gastric bypass (RYGB). These surgeries cause specific anatomic changes that promote weight loss; however, they also have unintended effects on the esophagus, particularly in terms of gastroesophageal reflux disease (GERD) and esophageal motility. Via restrictive surgery, LAGB has been widely reported to cause significant weight loss, although studies have also shown an increase and worsening of GERD as well as elevated rates of esophageal dilation, aperistalsis, and alterations in lower esophageal sphincter pressure. Along with LAGB, LSG has shown not only a worsening of GERD, but also the formation of de novo GERD in patients who were asymptomatic before the operation. In a restrictive-malabsorptive approach, RYGB has been reported to improve GERD and preserve esophageal motility. Bariatric surgery is a burgeoning field with immense implications on overall mortality. Future randomized, controlled trials are needed to better understand which patients should undergo particular surgeries, with greater emphasis on esophageal health and prevention of GERD and esophageal dysmotility.
Keywords: Laparoscopic adjustable gastric band; Roux-en-Y gastric bypass; bariatric surgery; esophageal dysmotility; gastroesophageal reflux disease; laparoscopic sleeve gastrectomy; obesity.
Figures
References
-
- Ford ES. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: a summary of the evidence. Diabetes Care. 2005;28(7):1769–2005. - PubMed
-
- Resnick HE, Jones K, Ruotolo G, et al. Strong Heart Study. Insulin resistance, the metabolic syndrome, and risk of incident cardiovascular disease in nondiabetic American Indians: the Strong Heart Study. Diabetes Care. 2003;26(3):861–2003. - PubMed
-
- Hamaguchi M, Kojima T, Takeda N, et al. The metabolic syndrome as a predictor of nonalcoholic fatty liver disease. Ann Intern Med. 2005;143(10):722–2005. - PubMed
-
- Aron-Wisnewsky J, Doré J, Clement K. The importance of the gut microbiota after bariatric surgery. Nat Rev Gastroenterol Hepatol. 2012;9(10):590–2012. - PubMed
-
- Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:i–xii. 1–253. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials