

Treatment of complex regional pain syndrome
- PMID: 27134629
- PMCID: PMC4832403
- DOI: 10.11138/ccmbm/2015.12.3s.026
Treatment of complex regional pain syndrome
Abstract
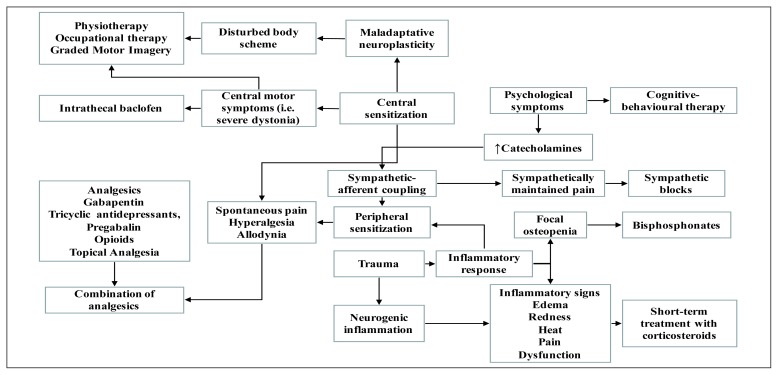
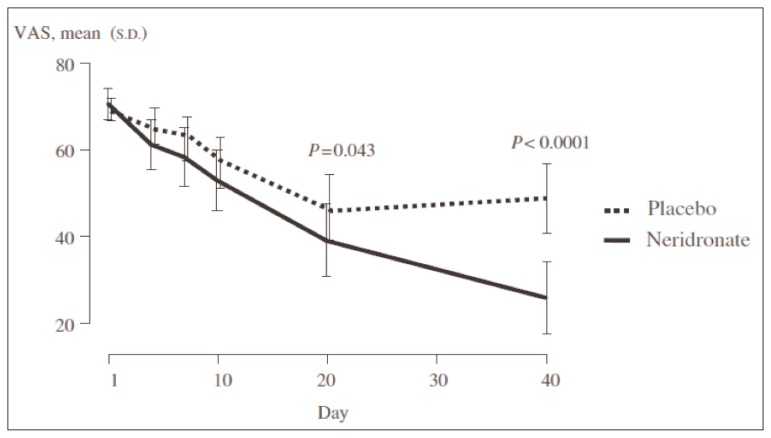
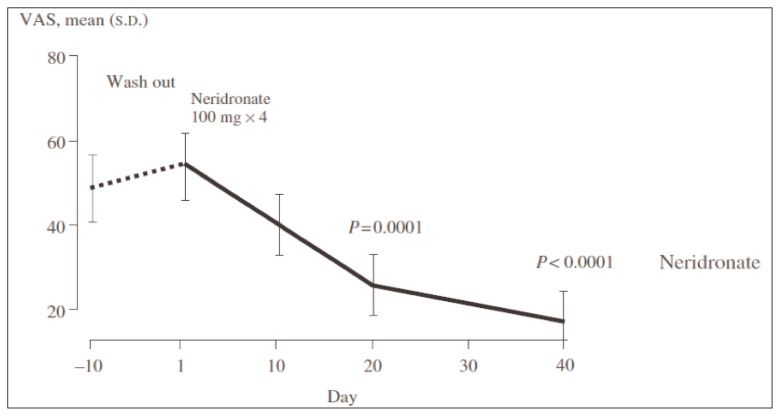
Complex Regional Pain Syndrome (CRPS) is a multifactorial and disabling disorder with complex etiology and pathogenesis. Goals of therapy in CRPS should be pain relief, functional restoration, and psychological stabilization, but early interventions are needed in order to achieve these objectives. Several drugs have been used to reduce pain and to improve functional status in CRPS, despite the lack of scientific evidence supporting their use in this scenario. They include anti-inflammatory drugs, analgesics, anesthetics, anticonvulsants, antidepressants, oral muscle relaxants, corticosteroids, calcitonin, bisphosphonates, calcium channel blockers and topical agents. NSAIDs showed no value in treating CRPS. Glucocorticoids are the only anti-inflammatory drugs for which there is direct clinical trial evidence in early stage of CRPS. Opioids are a reasonable second or third-line treatment option, but tolerance and long term toxicity are unresolved issues. The use of anticonvulsants and tricyclic antidepressants has not been well investigated for pain management in CRPS. During the last years, bisphosphonates have been the mostly studied pharmacologic agents in CRPS treatment and there are good evidence to support their use in this condition. Recently, the efficacy of intravenous (IV) administration of neridronate has been reported in a randomized controlled trial. Significant improvements in VAS score and other indices of pain and quality of life in patients who received four 100 mg IV doses of neridronate versus placebo were reported. These findings were confirmed in the open-extension phase of the study, when patients formerly enrolled in the placebo group received neridronate at the same dosage, and these results were maintained at 1 year follow-up. The current literature concerning sympathetic blocks and sympathectomy techniques lacks evidence of efficacy. Low evidence was recorded for a free radical scavenger, dimethylsulphoxide (DMSO) cream (50%). The same level of efficacy was noted for vitamin C (500 mg per day for 50 days) in prevention of CRPS in patients affected by wrist fracture. In conclusion, the best available therapeutic approach to CRPS is multimodal and is based on the use of several classes of drugs, associated to early physiotherapy. Neridronate at appropriate doses is associated with clinically relevant and persistent benefits in CRPS patients.
Keywords: complex regional pain syndrome; neridronate; pain management; therapy.
Figures
References
-
- Freedman M, Greis AC, Marino L, et al. Complex Regional Pain Syndrome. Diagnosis and Treatment. Phys Med Rehabil Clin N Am. 2014;25:291–303. - PubMed
-
- Gierthmuhlen J, Binder A, Baron R. Mechanism-based treatment in complex regional pain syndromes. Nat Rev Neurol. 2014;10(9):518–28. - PubMed
-
- Harden RN, Oaklander AL, Burton AW, et al. Complex Regional Pain Syndrome: practical diagnostic and treatment guidelines, 4th edition. Pain Medicine. 2013;14:180–229. - PubMed
-
- Rockett M. Diagnosis, mechanisms and treatment of complex regional pain syndrome. Curr Opin Anaesthesiol. 2014;27:494–500. - PubMed
-
- Rho RH, Brewer RP, Lamer TJ, et al. Complex regional pain syndrome. Mayo Clin Proc. 2002;77:174–80. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases