

Recent advances in understanding and managing cholestasis
- PMID: 27134744
- PMCID: PMC4841200
- DOI: 10.12688/f1000research.8012.1
Recent advances in understanding and managing cholestasis
Abstract
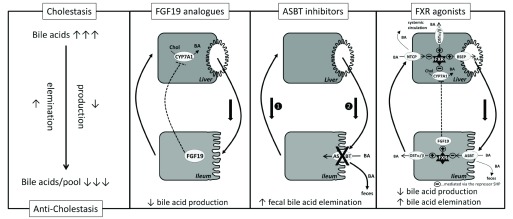
Cholestatic liver diseases are hereditary or acquired disorders with impaired hepatic excretion and enterohepatic circulation of bile acids and other cholephiles. The distinct pathological mechanisms, particularly for the acquired forms of cholestasis, are not fully revealed, but advances in the understanding of the molecular mechanisms and identification of key regulatory mechanisms of the enterohepatic circulation of bile acids have unraveled common and central mechanisms, which can be pharmacologically targeted. This overview focuses on the central roles of farnesoid X receptor, fibroblast growth factor 19, and apical sodium-dependent bile acid transporter for the enterohepatic circulation of bile acids and their potential as new drug targets for the treatment of cholestatic liver disease.
Keywords: bile acid; cholestasis; hepatic; liver.
Conflict of interest statement
Competing interests: Saul Karpen is an unpaid consultant for Intercept Pharmaceuticals.
No competing interests were disclosed.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources