

Endothelial ROS and Impaired Myocardial Oxygen Consumption in Sepsis-induced Cardiac Dysfunction
- PMID: 27135058
- PMCID: PMC4847432
- DOI: 10.21767/2471-8505.100020
Endothelial ROS and Impaired Myocardial Oxygen Consumption in Sepsis-induced Cardiac Dysfunction
Abstract
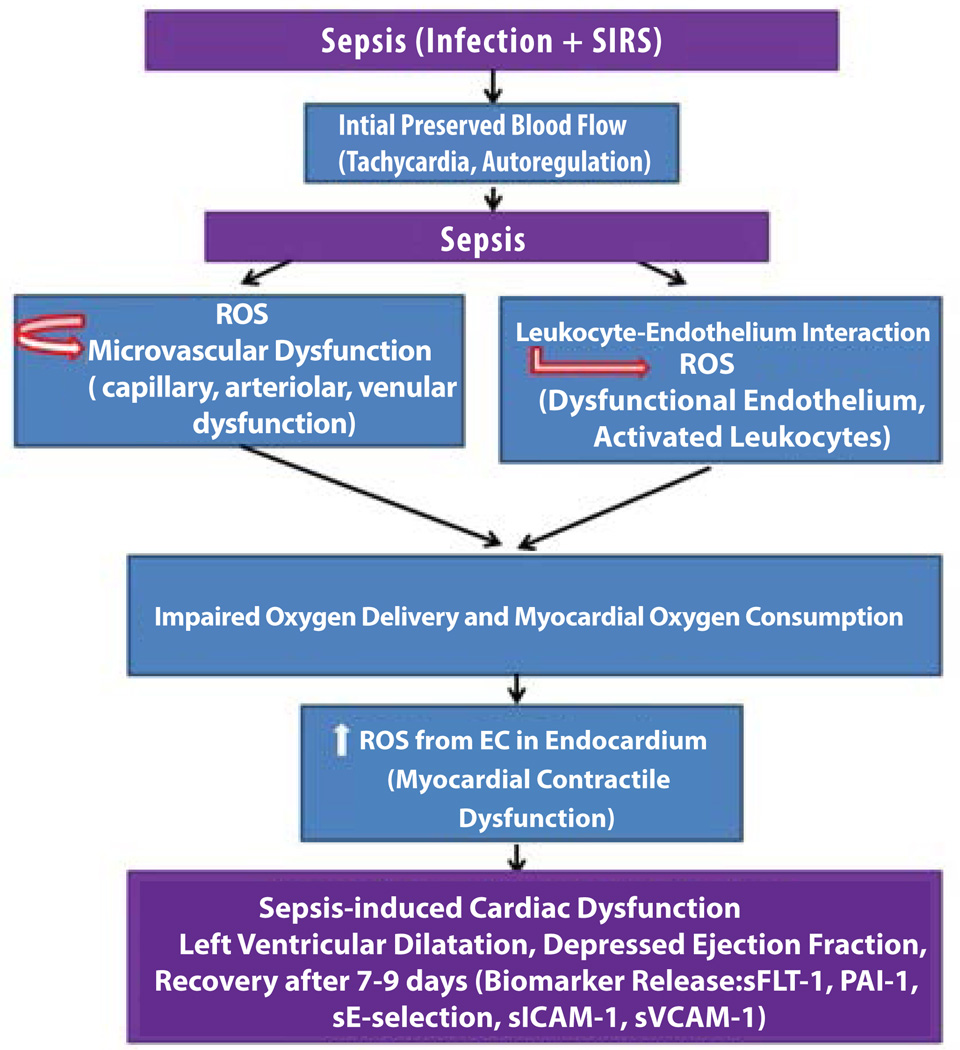
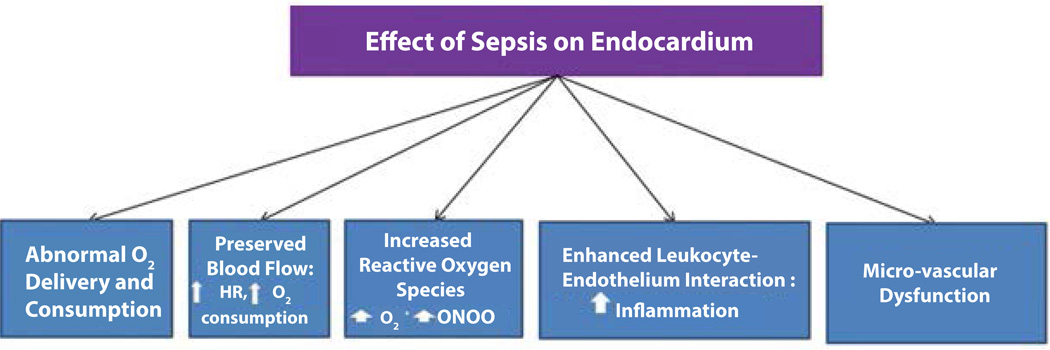
Sepsis is known as the presence of a Systemic Inflammatory Response Syndrome (SIRS) in response to an infection. In the USA alone, 750,000 cases of severe sepsis are diagnosed annually. More than 70% of sepsis-related deaths occur due to organ failure and more than 50% of septic patients demonstrate cardiac dysfunction. Patients with sepsis who develop cardiac dysfunction have significantly higher mortality, and thus cardiac dysfunction serves as a predictor of survival in sepsis. We have very little understanding about the mechanisms that result in cardiac dysfunction in the setting of sepsis. At present, the factors involved in sepsis-related cardiac dysfunction are believed to include the following: persistent inflammatory changes in the vascular endothelium and endocardium leading to circulatory and micro vascular changes, increase in endothelial reactive oxygen species (ROS), abnormal endothelium-leukocyte interaction resulting in a feed-forward loop for inflammatory cytokines and ROS, contractile dysfunction of the heart due to autonomic dysregulation, metabolic changes in myocardium leading to impaired oxygen delivery and increased oxygen consumption, mitochondrial dysfunction, and persistent inflammatory signaling. In this review article, we will briefly discuss the clinical challenges and our current understanding of cardiac dysfunction in sepsis. Major focus will be on the pathological changes that occur in vascular endothelium, with an emphasis on endocardium, and how endothelial ROS, impaired endothelium-leukocyte interaction, and microcirculatory changes lead to cardiac dysfunction in sepsis. The importance of the ongoing quest for the clinical biomarkers for cardiac dysfunction will also be discussed.
Keywords: Biomarker; Cardiac dysfunction; Endothelium; Microvascular dysfunction; Reactive oxygen species (ROS); Sepsis.
Figures
Similar articles
-
A burning issue: do sepsis and systemic inflammatory response syndrome (SIRS) directly contribute to cardiac dysfunction?Front Biosci. 2006 Jan 1;11:15-22. doi: 10.2741/1776. Front Biosci. 2006. PMID: 16146710 Review.
-
Oxidative stress and endothelial dysfunction during sepsis.Front Biosci (Landmark Ed). 2011 Jan 1;16(5):1986-95. doi: 10.2741/3835. Front Biosci (Landmark Ed). 2011. PMID: 21196278 Review.
-
Sepsis Care Pathway 2019.Qatar Med J. 2019 Nov 7;2019(2):4. doi: 10.5339/qmj.2019.qccc.4. eCollection 2019. Qatar Med J. 2019. PMID: 31763206 Free PMC article.
-
[Role of microcirculation in multiorgan failure of infectious origin].Bull Acad Natl Med. 2000;184(8):1609-19; discussion 1619-20. Bull Acad Natl Med. 2000. PMID: 11471382 Review. French.
-
Myocardial contractile dysfunction in the systemic inflammatory response syndrome: role of a cytokine-inducible nitric oxide synthase in cardiac myocytes.J Mol Cell Cardiol. 1995 Jan;27(1):155-67. doi: 10.1016/s0022-2828(08)80015-6. J Mol Cell Cardiol. 1995. PMID: 7539082 Review.
Cited by
-
Sepsis-Pathophysiology and Therapeutic Concepts.Front Med (Lausanne). 2021 May 14;8:628302. doi: 10.3389/fmed.2021.628302. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34055825 Free PMC article. Review.
-
The potential mechanism of mitochondrial dysfunction in septic cardiomyopathy.J Int Med Res. 2018 Jun;46(6):2157-2169. doi: 10.1177/0300060518765896. Epub 2018 Apr 11. J Int Med Res. 2018. PMID: 29637807 Free PMC article.
-
Corylin alleviated sepsis-associated cardiac dysfunction via attenuating inflammation through downregulation of microRNA-214-5p.Toxicol Res (Camb). 2024 Jun 7;13(3):tfae081. doi: 10.1093/toxres/tfae081. eCollection 2024 Jun. Toxicol Res (Camb). 2024. PMID: 38855635 Free PMC article.
-
Novel Insights Into the Potential Mechanisms of N6-Methyladenosine RNA Modification on Sepsis-Induced Cardiovascular Dysfunction: An Update Summary on Direct and Indirect Evidences.Front Cell Dev Biol. 2021 Nov 12;9:772921. doi: 10.3389/fcell.2021.772921. eCollection 2021. Front Cell Dev Biol. 2021. PMID: 34869371 Free PMC article. Review.
-
Epigallocatechin-3-gallate protects sepsis-induced myocardial dysfunction by inhibiting the nuclear factor-κB signaling pathway.Heliyon. 2024 Feb 27;10(5):e27163. doi: 10.1016/j.heliyon.2024.e27163. eCollection 2024 Mar 15. Heliyon. 2024. PMID: 38449632 Free PMC article.
References
-
- Furian T, Aguiar C, Prado K, Ribeiro RV, Becker L, et al. Ventricular dysfunction and dilation in severe sepsis and septic shock: Relation to endothelial function and mortality. J Crit Care. 2012;27:e9–e15. - PubMed
-
- Hochstadt A, Meroz Y, Landesberg G. Myocardial dysfunction in severe sepsis and septic shock: More questions than answers? J Cardiothorac Vasc Anesth. 2011;25:526–535. - PubMed
-
- Committee M of the AC of CP of CCMCC. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: Definitions for Sepsis and Organ Failure and Guidelines for the Use of Innovative Therapies in Sepsis. Crit Care Med Care Med. 1992;20:864–874. - PubMed
-
- Zaky A, Deem S, Bendjelid K, Treggiari MM. Characterization of cardiac dysfunction in sepsis: an ongoing challenge. Shock. 2014;41:12–24. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources