

Young Adult Exposure to Cardiovascular Risk Factors and Risk of Events Later in Life: The Framingham Offspring Study
- PMID: 27138014
- PMCID: PMC4854462
- DOI: 10.1371/journal.pone.0154288
Young Adult Exposure to Cardiovascular Risk Factors and Risk of Events Later in Life: The Framingham Offspring Study
Abstract
Background: It is unclear whether coronary heart disease (CHD) risk factor exposure during early adulthood contributes to CHD risk later in life. Our objective was to analyze whether extent of early adult exposures to systolic and diastolic blood pressure (SBP, DBP) and low-and high-density lipoprotein cholesterol (LDL, HDL) are independent predictors of CHD events later in life.
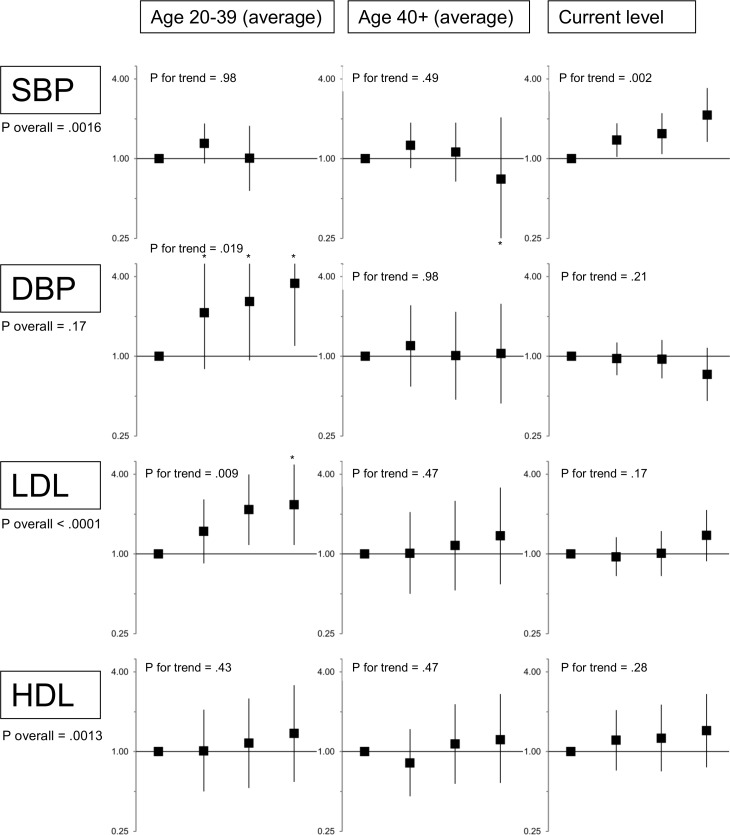
Methods and findings: We used all available measurements of SBP, DBP, LDL, and HDL collected over 40 years in the Framingham Offspring Study to estimate risk factor trajectories, starting at age 20 years, for all participants. Average early adult (age 20-39) exposure to each risk factor was then estimated, and used to predict CHD events (myocardial infarction or CHD death) after age 40, with adjustment for risk factor exposures later in life (age 40+). 4860 participants contributed an average of 6.3 risk factor measurements from in-person examinations and 24.5 years of follow-up after age 40, and 510 had a first CHD event. Early adult exposures to high SBP, DBP, LDL or low HDL were associated with 8- to 30-fold increases in later life CHD event rates, but were also strongly correlated with risk factor levels later in life. After adjustment for later life levels and other risk factors, early adult DBP and LDL remained strongly associated with later life risk. Compared with DBP≤70 mmHg, adjusted hazard ratios (HRs) were 2.1 (95% confidence interval: 0.8-5.7) for DBP = 71-80, 2.6 (0.9-7.2) for DBP = 81-90, and 3.6 (1.2-11) for DBP>90 (p-trend = 0.019). Compared with LDL≤100 mg/dl, adjusted HRs were 1.5 (0.9-2.6) for LDL = 101-130, 2.2 (1.2-4.0) for LDL = 131-160, and 2.4 (1.2-4.7) for LDL>160 (p-trend = 0.009). While current levels of SBP and HDL were also associated with CHD events, we did not detect an independent association with early adult exposure to either of these risk factors.
Conclusions: Using a mixed modeling approach to estimation of young adult exposures with trajectory analysis, we detected independent associations between estimated early adult exposures to non-optimal DBP and LDL and CHD events later in life.
Conflict of interest statement
Figures
References
-
- Vasan RS, Larson MG, Leip EP, Evans JC, O'Donnell CJ, Kannel WB, et al. Impact of high-normal blood pressure on the risk of cardiovascular disease. The New England journal of medicine. 2001;345(18):1291–7. - PubMed
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–13. - PubMed
-
- Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366(9493):1267–78. - PubMed
-
- Mihaylova B, Emberson J, Blackwell L, Keech A, Simes J, Barnes EH, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012;380(9841):581–90. 10.1016/S0140-6736(12)60367-5 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
