

Safe and Efficient Gene Therapy for Pyruvate Kinase Deficiency
- PMID: 27138040
- PMCID: PMC5088764
- DOI: 10.1038/mt.2016.87
Safe and Efficient Gene Therapy for Pyruvate Kinase Deficiency
Abstract
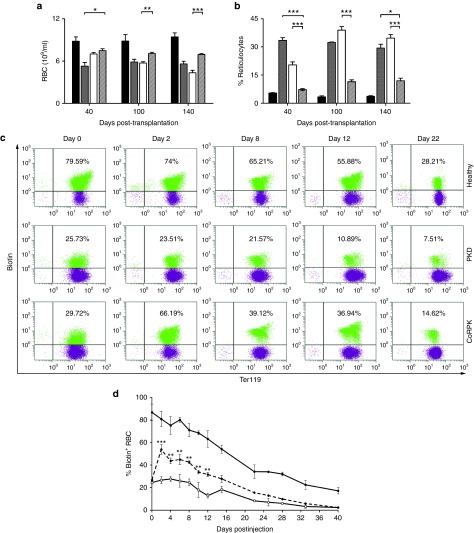
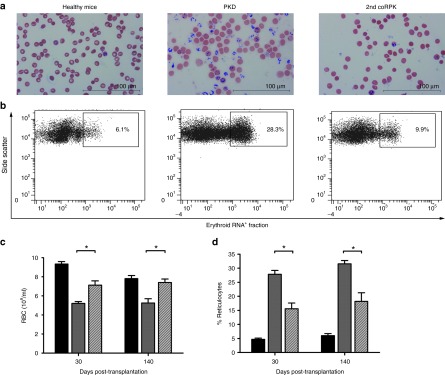
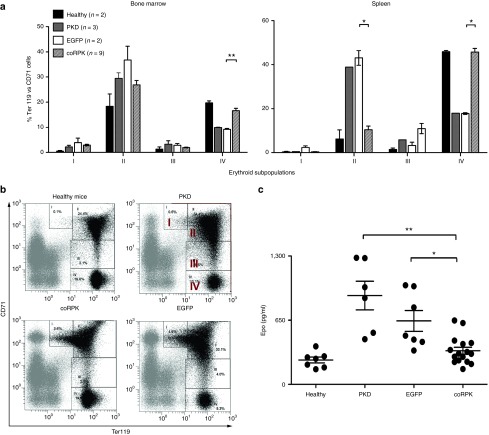
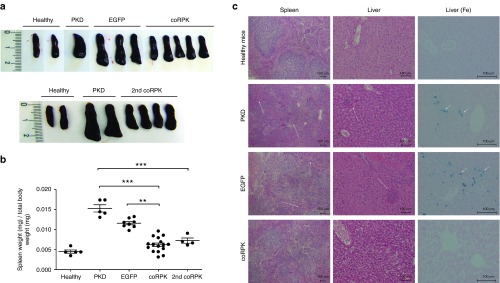
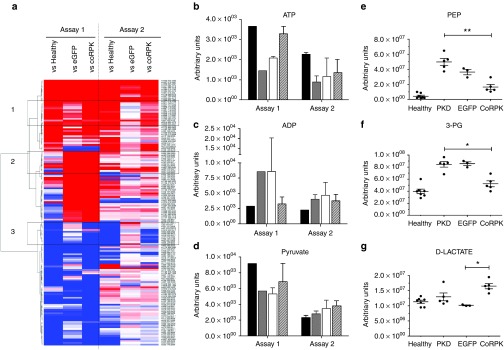
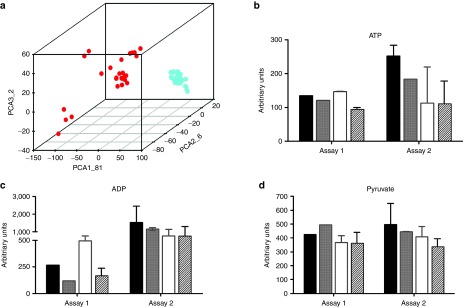
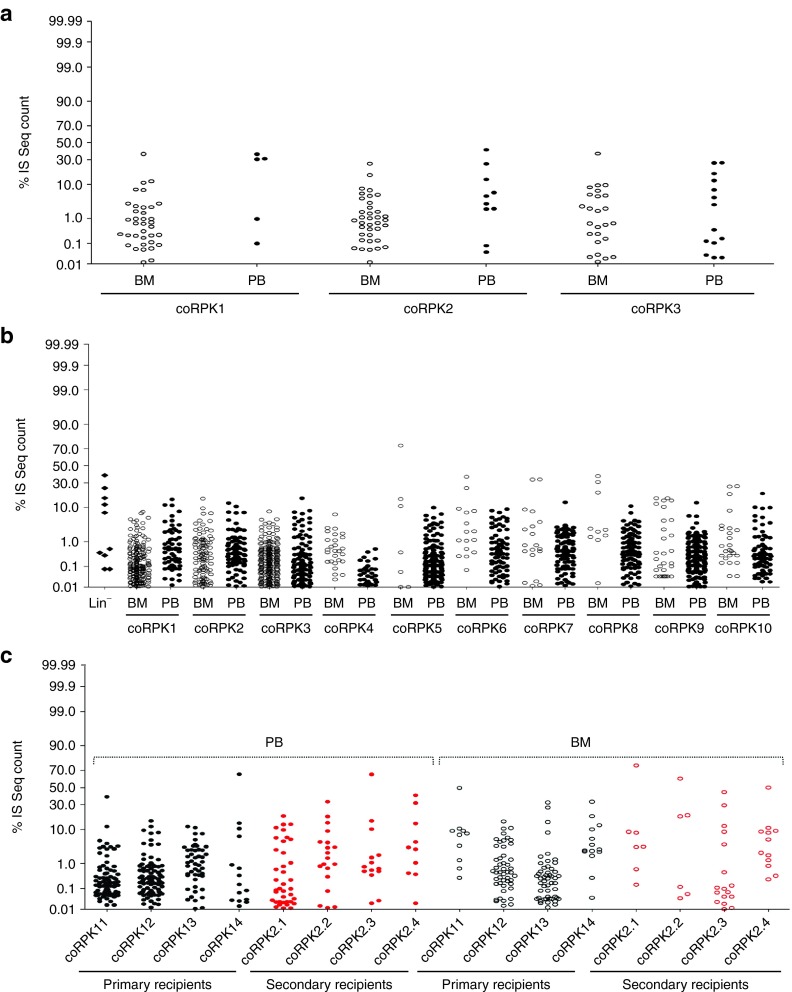
Pyruvate kinase deficiency (PKD) is a monogenic metabolic disease caused by mutations in the PKLR gene that leads to hemolytic anemia of variable symptomatology and that can be fatal during the neonatal period. PKD recessive inheritance trait and its curative treatment by allogeneic bone marrow transplantation provide an ideal scenario for developing gene therapy approaches. Here, we provide a preclinical gene therapy for PKD based on a lentiviral vector harboring the hPGK eukaryotic promoter that drives the expression of the PKLR cDNA. This therapeutic vector was used to transduce mouse PKD hematopoietic stem cells (HSCs) that were subsequently transplanted into myeloablated PKD mice. Ectopic RPK expression normalized the erythroid compartment correcting the hematological phenotype and reverting organ pathology. Metabolomic studies demonstrated functional correction of the glycolytic pathway in RBCs derived from genetically corrected PKD HSCs, with no metabolic disturbances in leukocytes. The analysis of the lentiviral insertion sites in the genome of transplanted hematopoietic cells demonstrated no evidence of genotoxicity in any of the transplanted animals. Overall, our results underscore the therapeutic potential of the hPGK-coRPK lentiviral vector and provide high expectations toward the gene therapy of PKD and other erythroid metabolic genetic disorders.
Figures
References
-
- Zanella, A, Bianchi, P and Fermo, E (2007). Pyruvate kinase deficiency. Haematologica 92: 721–723. - PubMed
-
- Pissard, S, Max-Audit, I, Skopinski, L, Vasson, A, Vivien, P, Bimet, C et al. (2006). Pyruvate kinase deficiency in France: a 3-year study reveals 27 new mutations. Br J Haematol 133: 683–689. - PubMed
-
- Beutler, E and Gelbart, T (2000). Estimating the prevalence of pyruvate kinase deficiency from the gene frequency in the general white population. Blood 95: 3585–3588. - PubMed
-
- Tanphaichitr, VS, Suvatte, V, Issaragrisil, S, Mahasandana, C, Veerakul, G, Chongkolwatana, V et al. (2000). Successful bone marrow transplantation in a child with red blood cell pyruvate kinase deficiency. Bone Marrow Transplant 26: 689–690. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
