

Pembrolizumab in Patients With Advanced Triple-Negative Breast Cancer: Phase Ib KEYNOTE-012 Study
- PMID: 27138582
- PMCID: PMC6816000
- DOI: 10.1200/JCO.2015.64.8931
Pembrolizumab in Patients With Advanced Triple-Negative Breast Cancer: Phase Ib KEYNOTE-012 Study
Abstract
Purpose: Immune checkpoint inhibition has been demonstrated to be an effective anticancer strategy. Several lines of evidence support the study of immunotherapy in triple-negative breast cancer (TNBC). We assessed the safety and antitumor activity of the programmed cell death protein 1 (PD-1) inhibitor pembrolizumab in patients with advanced TNBC.
Methods: KEYNOTE-012 (ClinicalTrials.gov identifier: NCT01848834) was a multicenter, nonrandomized phase Ib trial of single-agent pembrolizumab given intravenously at 10 mg/kg every 2 weeks to patients with advanced PD-L1-positive (expression in stroma or ≥ 1% of tumor cells by immunohistochemistry) TNBC, gastric cancer, urothelial cancer, and head and neck cancer. This report focuses on the TNBC cohort.
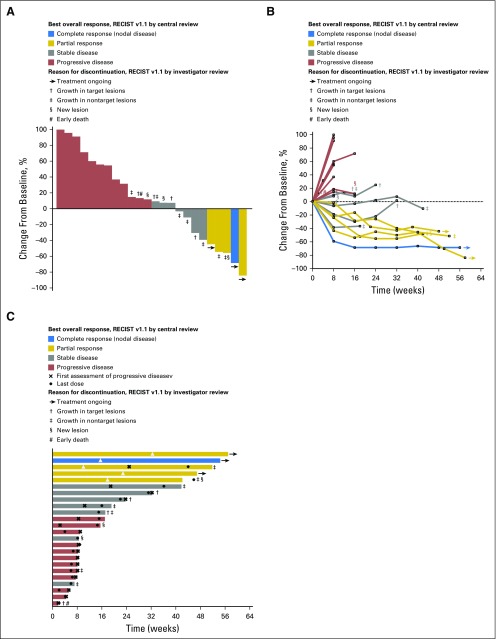
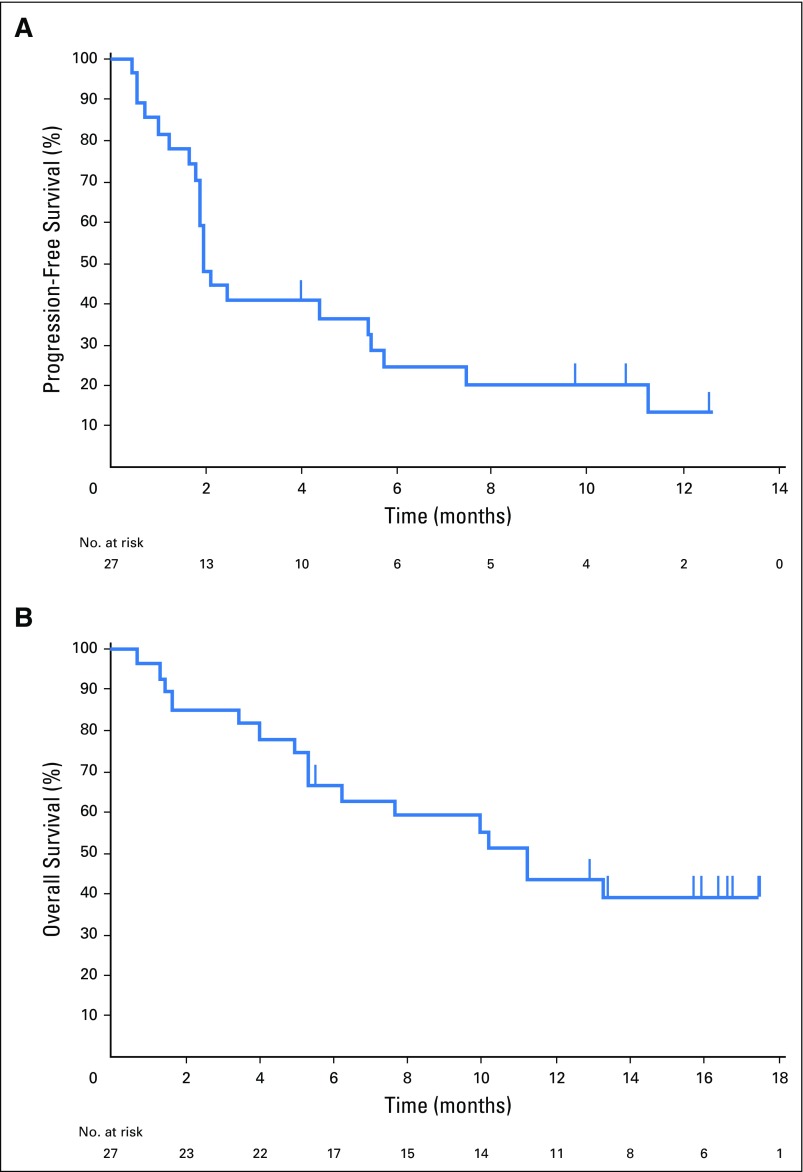
Results: Among 111 patients with TNBC whose tumor samples were screened for PD-L1 expression, 58.6% had PD-L1-positive tumors. Thirty-two women (median age, 50.5 years; range, 29 to 72 years) were enrolled and assessed for safety and antitumor activity. The median number of doses administered was five (range, 1 to 36 doses). Common toxicities were mild and similar to those observed in other tumor cohorts (eg, arthralgia, fatigue, myalgia, and nausea), and included five (15.6%) patients with grade ≥ 3 toxicity and one treatment-related death. Among the 27 patients who were evaluable for antitumor activity, the overall response rate was 18.5%, the median time to response was 17.9 weeks (range, 7.3 to 32.4 weeks), and the median duration of response was not yet reached (range, 15.0 to ≥ 47.3 weeks).
Conclusion: This phase Ib study describes preliminary evidence of clinical activity and a potentially acceptable safety profile of pembrolizumab given every 2 weeks to patients with heavily pretreated, advanced TNBC. A single-agent phase II study examining a 200-mg dose given once every 3 weeks (ClinicalTrials.gov identifier: NCT02447003) is ongoing.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
References
-
- Foulkes WD, Smith IE, Reis-Filho JS: Triple-negative breast cancer. N Engl J Med 363:1938–1948,2010 - PubMed
-
- Dent R Trudeau M Pritchard KI, etal: Triple-negative breast cancer: Clinical features and patterns of recurrence. Clin Cancer Res 13:4429–4434,2007 - PubMed
-
- American Cancer Society : American Cancer Society Breast Cancer Facts and Figures 2013-2014 2013. Atlanta, GA: American Cancer Society
-
- Rakha EA Elsheikh SE Aleskandarany MA, etal: Triple-negative breast cancer: Distinguishing between basal and nonbasal subtypes. Clin Cancer Res 15:2302–2310,2009 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
