

Risk of Advanced Neoplasia in First-Degree Relatives with Colorectal Cancer: A Large Multicenter Cross-Sectional Study
- PMID: 27138769
- PMCID: PMC4854417
- DOI: 10.1371/journal.pmed.1002008
Risk of Advanced Neoplasia in First-Degree Relatives with Colorectal Cancer: A Large Multicenter Cross-Sectional Study
Abstract
Background: First-degree relatives (FDR) of patients with colorectal cancer have a higher risk of developing colorectal cancer than the general population. For this reason, screening guidelines recommend colonoscopy every 5 or 10 y, starting at the age of 40, depending on whether colorectal cancer in the index-case is diagnosed at <60 or ≥60 y, respectively. However, studies on the risk of neoplastic lesions are inconclusive. The aim of this study was to determine the risk of advanced neoplasia (three or more non-advanced adenomas, advanced adenoma, or invasive cancer) in FDR of patients with colorectal cancer compared to average-risk individuals (i.e., asymptomatic adults 50 to 69 y of age with no family history of colorectal cancer).
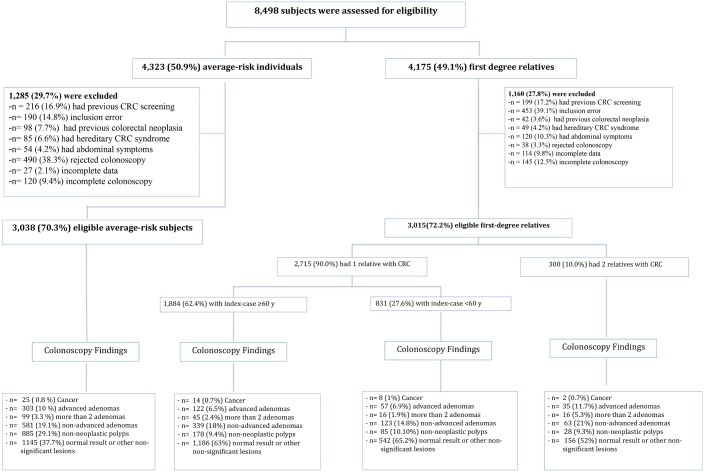
Methods and findings: This cross-sectional analysis includes data from 8,498 individuals undergoing their first lifetime screening colonoscopy between 2006 and 2012 at six Spanish tertiary hospitals. Of these individuals, 3,015 were defined as asymptomatic FDR of patients with colorectal cancer ("familial-risk group") and 3,038 as asymptomatic with average-risk for colorectal cancer ("average-risk group"). The familial-risk group was stratified as one FDR, with one family member diagnosed with colorectal cancer at ≥60 y (n = 1,884) or at <60 y (n = 831), and as two FDR, with two family members diagnosed with colorectal cancer at any age (n = 300). Multiple logistic regression analysis was used for between-group comparisons after adjusting for potential confounders (age, gender, and center). Compared with the average-risk group, advanced neoplasia was significantly more prevalent in individuals having two FDR with colorectal cancer (odds ratio [OR] 1.90; 95% confidence interval [CI] 1.36-2.66, p < 0.001), but not in those having one FDR with colorectal cancer diagnosed at ≥60 y (OR 1.03; 95% CI 0.83-1.27, p = 0.77) and <60 y (OR 1.19; 95% CI 0.90-1.58, p = 0.20). After the age of 50 y, men developed advanced neoplasia over two times more frequently than women and advanced neoplasia appeared at least ten y earlier. Fewer colonoscopies by 2-fold were required to detect one advanced neoplasia in men than in women. Major limitations of this study were first that although average-risk individuals were consecutively included in a randomized control trial, this was not the case for all individuals in the familial-risk cohort; and second, the difference in age between the average-risk and familial-risk cohorts.
Conclusions: Individuals having two FDR with colorectal cancer showed an increased risk of advanced neoplasia compared to those with average-risk for colorectal cancer. Men had over 2-fold higher risk of advanced neoplasia than women, independent of family history. These data suggest that screening colonoscopy guidelines should be revised in the familial-risk population.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Lieberman DA, Rex DK, Winawer SJ, Giardiello FM, Johnson DA, Levin TR. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012;143(3):844–57. Epub 2012/07/06. 10.1053/j.gastro.2012.06.001 . - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
