

Exercise and load modification versus corticosteroid injection versus 'wait and see' for persistent gluteus medius/minimus tendinopathy (the LEAP trial): a protocol for a randomised clinical trial
- PMID: 27139495
- PMCID: PMC4852446
- DOI: 10.1186/s12891-016-1043-6
Exercise and load modification versus corticosteroid injection versus 'wait and see' for persistent gluteus medius/minimus tendinopathy (the LEAP trial): a protocol for a randomised clinical trial
Abstract
Background: Lateral hip pain is common, particularly in females aged 40-60 years. The pain can affect sleep and daily activities, and is frequently recalcitrant. The condition is often diagnosed as trochanteric bursitis, however radiological and surgical studies have revealed that the most common pathology is gluteus medius/minimus tendinopathy. Patients are usually offered three treatment options: (a) corticosteroid injection (CSI), (b) physiotherapy, or (c) reassurance and observation. Research on Achilles and patellar tendons has shown that load modification and exercise appears to be more effective than other treatments for managing tendinopathy, however, it is unclear whether a CSI, or a load modification and exercise-based physiotherapy approach is more effective in gluteal tendinopathy. This randomised controlled trial aims to compare the efficacy on pain and function of a load modification and exercise-based programme with a CSI and a 'wait and see' approach for gluteal tendinopathy.
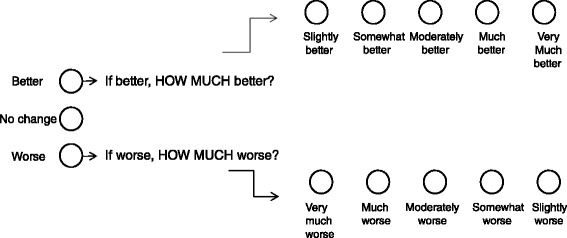
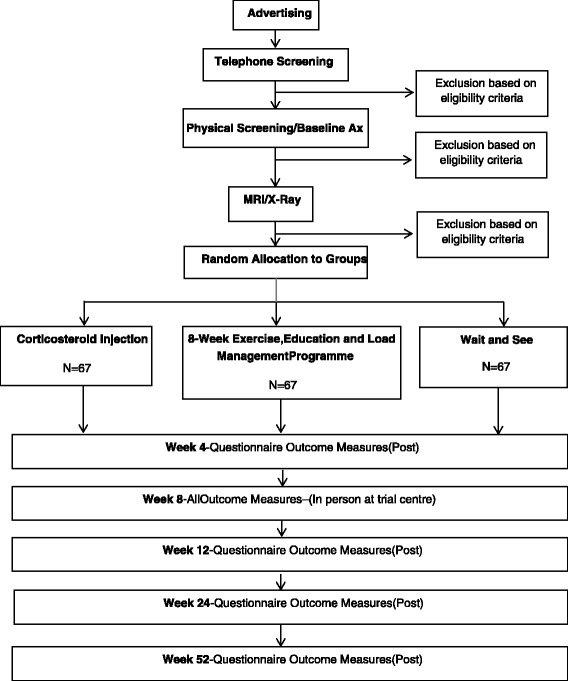
Methods: Two hundred one people with gluteal tendinopathy will be randomly allocated into one of three groups: (i) CSI; (ii) physiotherapist-administered load modification and exercise intervention; and (iii) wait and see approach. The CSI therapy will consist of one ultrasound (US) guided CSI around the affected tendons and advice on tendon care. Education about load modification will be delivered in physiotherapy clinics and the exercise programme will be both home-based and supervised. The group allocated the wait and see approach will receive basic tendon care advice and reassurance in a single session by a trial physiotherapist. Outcomes will be evaluated at baseline, 4, 8, 12, 26 and 52 weeks using validated global rating of change, pain and physical function scales, psychological measures, quality of life and physical activity levels. Hip abductor muscle strength will be measured at baseline and 8 weeks. Economic evaluation will be performed to investigate the cost-effectiveness of the active interventions compared with the wait and see approach. Analyses will be conducted on an intention-to-treat basis using logistic and linear mixed regression models and the economic evaluation will report incremental cost-utility ratios. The trial reporting will comply with CONSORT guidelines.
Discussion: This study will provide clinicians with directly applicable evidence of the relative efficacy of three common approaches to the management of gluteal tendinopathy.
Trial registration: Australia New Zealand Clinical Trials Registry ACTRN12612001126808. Date Registered: 22/10/2012.
Keywords: Corticosteroid injection; Gluteal tendinopathy; Greater trochanteric pain syndrome; Physiotherapy.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
