

Clinical study of midazolam sequential with dexmedetomidine for agitated patients undergoing weaning to implement light sedation in intensive care unit
- PMID: 27140216
- PMCID: PMC4897849
- DOI: 10.1016/j.cjtee.2015.09.007
Clinical study of midazolam sequential with dexmedetomidine for agitated patients undergoing weaning to implement light sedation in intensive care unit
Abstract
Purpose: To evaluate midazolam sequential with dexmedetomidine for agitated patients undergoing weaning to implement light sedation in ICU.
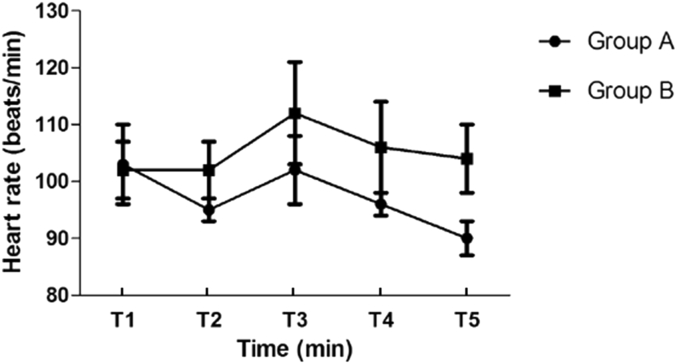
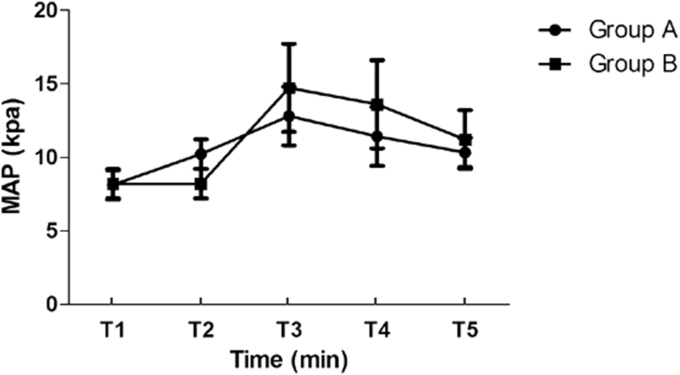
Methods: This randomized, prospective study was conducted in Tianjin Third Central Hospital, China. Using a sealed-envelope method, the patients were randomly divided into 2 groups (40 patients per group). Each patient of group A received an initial loading dose of midazolam at 0.3-3mg/kg·h 24 h before extubation, followed by an infusion of dexmedetomidine at a rate of 0.2-1 μg/kg·h until extubation. Each patient of group B received midazolam at a dose of 0.3-3 mg/kg·h until extubation. The dose of sedation was regulated according to RASS sedative scores maintaining in the range of -2-1. All patients were continuously monitored for 60 min after extubation. During the course, heart rate (HR), mean artery pressure (MAP), extubation time, adverse reactions, ICU stay, and hospital stay were observed and recorded continuously at the following time points: 24 h before extubation (T1), 12 h before extubation (T2), extubation (T3), 30 min after extubation (T4), 60 min after extubation (T5).
Results: Both groups reached the goal of sedation needed for ICU patients. Dexmedetomidine was associated with a significant increase in extubation quality compared with midazolam, reflected in the prevalence of delirium after extubation (20% (8/40) vs 45% (18/40)), respectively (p= 0.017). There were no clinically significant decreases in HR and MAP after infusing dexmedetomidine or midazolam. In the group A, HR was not significantly increased after extubation; however, in the group B, HR was significantly increased compared with the preextubation values (p < 0.05). HR was significantly higher in the group B compared with the group A at 30 and 60 min after extubation (both, p <0.05). Compared with preextubation values, MAP was significantly increased at extubation in the group B (p < 0.05) and MAP was significantly higher at T3, T4, T5 in the group B than group A (p < 0.05). There was a significant difference in extubation time ((3.0 ± 1.5) d vs (4.3 ± 2.2) d, p < 0.05), ICU stay ((5.4 ± 2.1) d vs (8.0 ± 1.4) d, p < 0.05), hospital stay ((10.1 ± 3.0) d vs (15.3 ± 2.6) d, p <0.05) between group A and B.
Conclusion: Midazolam sequential with dexmedetomidine can reach the goal of sedation for ICU agitated patients, meanwhile it can maintain the respiratory and circulation parameters and reduce adverse reactions.
Figures
Similar articles
-
[A study of using dexmedetomidine in ventilator bundle treatment in an ICU].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015 Oct;27(10):836-40. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015. PMID: 27132448 Clinical Trial. Chinese.
-
Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial.JAMA. 2009 Feb 4;301(5):489-99. doi: 10.1001/jama.2009.56. Epub 2009 Feb 2. JAMA. 2009. PMID: 19188334 Clinical Trial.
-
Prolonged sedation of critically ill patients with midazolam or propofol: impact on weaning and costs.Crit Care Med. 1997 Jan;25(1):33-40. doi: 10.1097/00003246-199701000-00009. Crit Care Med. 1997. PMID: 8989173 Clinical Trial.
-
Effectiveness of dexmedetomidine versus propofol on extubation times, length of stay and mortality rates in adult cardiac surgery patients: a systematic review and meta-analysis.JBI Database System Rev Implement Rep. 2018 May;16(5):1220-1239. doi: 10.11124/JBISRIR-2017-003488. JBI Database System Rev Implement Rep. 2018. PMID: 29762314
-
A comparation of dexmedetomidine and midazolam for sedation in patients with mechanical ventilation in ICU: A systematic review and meta-analysis.PLoS One. 2023 Nov 14;18(11):e0294292. doi: 10.1371/journal.pone.0294292. eCollection 2023. PLoS One. 2023. PMID: 37963140 Free PMC article.
Cited by
-
A systematic review of interventions to facilitate extubation in patients difficult-to-wean due to delirium, agitation, or anxiety and a meta-analysis of the effect of dexmedetomidine.Can J Anaesth. 2019 Mar;66(3):318-327. doi: 10.1007/s12630-018-01289-1. Epub 2019 Jan 23. Can J Anaesth. 2019. PMID: 30674004 English.
-
The Japanese Clinical Practice Guidelines for Management of Sepsis and Septic Shock 2020 (J-SSCG 2020).J Intensive Care. 2021 Aug 25;9(1):53. doi: 10.1186/s40560-021-00555-7. J Intensive Care. 2021. PMID: 34433491 Free PMC article.
-
The Japanese Clinical Practice Guidelines for Management of Sepsis and Septic Shock 2020 (J-SSCG 2020).Acute Med Surg. 2021 Aug 26;8(1):e659. doi: 10.1002/ams2.659. eCollection 2021 Jan-Dec. Acute Med Surg. 2021. PMID: 34484801 Free PMC article.
References
-
- Ngwenyama N.E., Anderson J., Hoernschemeyer D.G. Effects of dexmedetomidine on propofol and remifentanil infusion rates during total intravenous anesthesia for spine surgery in adolescents. Paediatr Anaesth. 2008;18:1190–1195. - PubMed
-
- Bulow N.M., Barbosa N.V., Rocha J.B. Opioid consumption in total intravenous anesthesia is reduced with dexmedetomidine: a comparative study with remifentanil in gynecologic videolaparoscopic surgery. J Clin Anesth. 2007;19:280–285. - PubMed
-
- Jaakola M.L., Ali-Melkkilä T., Kanto J. Dexmedetomidine reduces intraocular pressure, intubation responses and anaesthetic requirements in patients undergoing ophthalmic surgery. Br J Anaesth. 1992;68:570–575. - PubMed
-
- Talke P., Chen R., Thomas B. The hemodynamic and adrenergic effects of perioperative dexmedetomidine infusion after vascular surgery. Anesth Analg. 2000;90:834–839. - PubMed
-
- Milbrandt E.B., Deppen S., Harrison P.L. Costs associated with delirium in mechanically ventilated patients. Crit Care Med. 2004;32:955–962. - PubMed