

Diagnostic performance of cardiac imaging methods to diagnose ischaemia-causing coronary artery disease when directly compared with fractional flow reserve as a reference standard: a meta-analysis
- PMID: 27141095
- PMCID: PMC5381594
- DOI: 10.1093/eurheartj/ehw095
Diagnostic performance of cardiac imaging methods to diagnose ischaemia-causing coronary artery disease when directly compared with fractional flow reserve as a reference standard: a meta-analysis
Abstract
Aims: The aim of this study was to determine the diagnostic performance of single-photon emission computed tomography (SPECT), stress echocardiography (SE), invasive coronary angiography (ICA), coronary computed tomography angiography (CCTA), fractional flow reserve (FFR) derived from CCTA (FFRCT), and cardiac magnetic resonance (MRI) imaging when directly compared with an FFR reference standard.
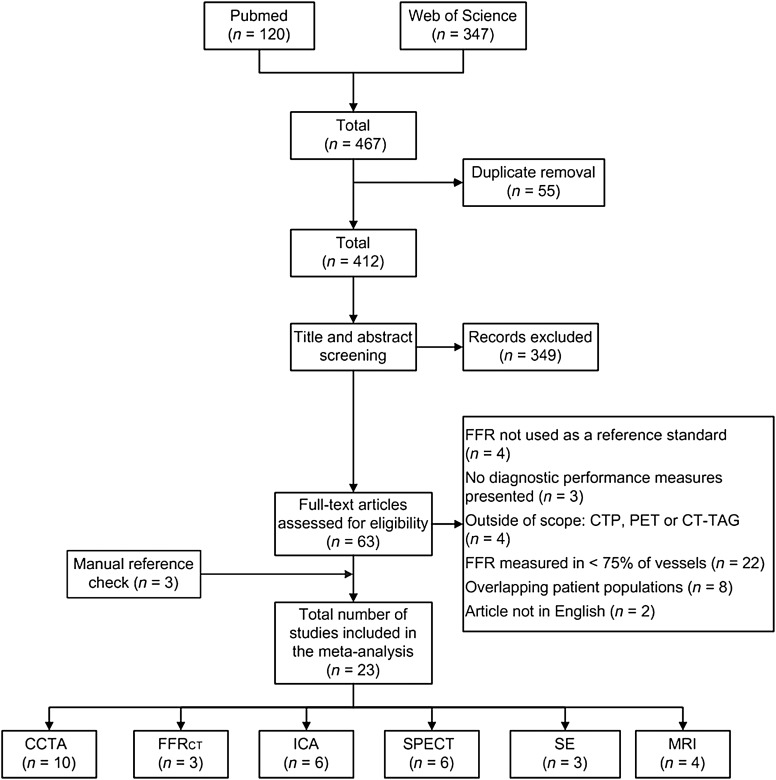
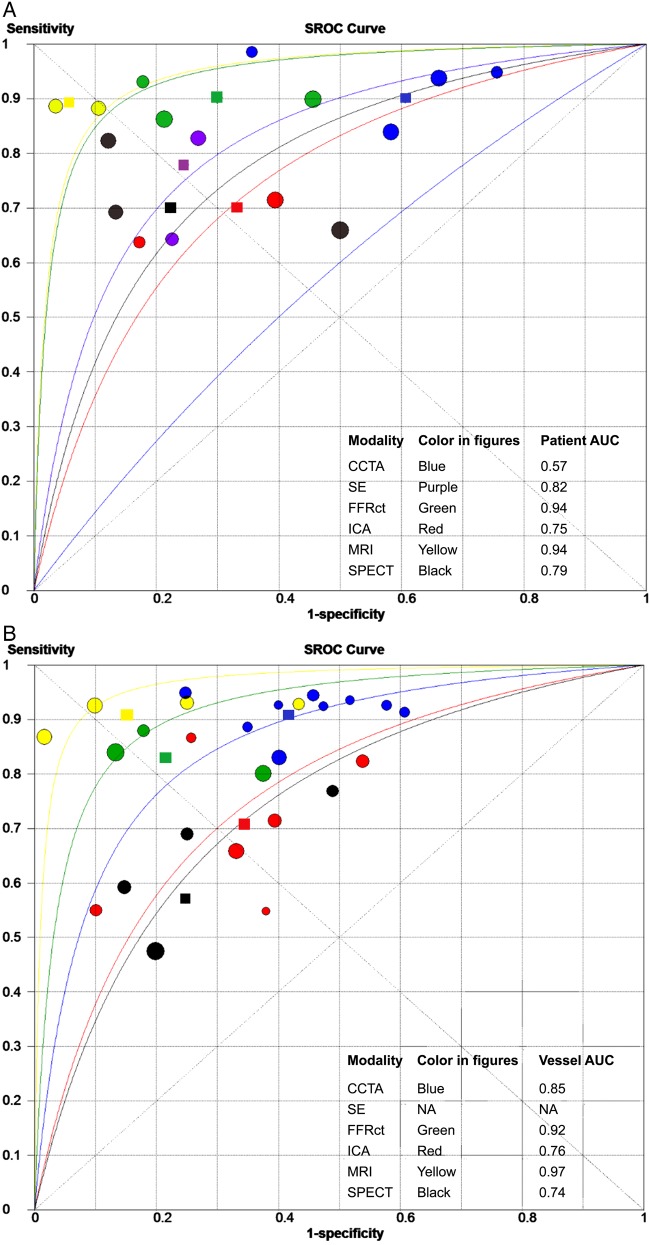
Method and results: PubMed and Web of Knowledge were searched for investigations published between 1 January 2002 and 28 February 2015. Studies performing FFR in at least 75% of coronary vessels for the diagnosis of ischaemic coronary artery disease (CAD) were included. Twenty-three articles reporting on 3788 patients and 5323 vessels were identified. Meta-analysis was performed for pooled sensitivity, specificity, likelihood ratios (LR), diagnostic odds ratio, and summary receiver operating characteristic curves. In contrast to ICA, CCTA, and FFRCT reports, studies evaluating SPECT, SE, and MRI were largely retrospective, single-centre and with generally smaller study samples. On a per-patient basis, the sensitivity of CCTA (90%, 95% CI: 86-93), FFRCT (90%, 95% CI: 85-93), and MRI (90%, 95% CI: 75-97) were higher than for SPECT (70%, 95% CI: 59-80), SE (77%, 95% CI: 61-88), and ICA (69%, 95% CI: 65-75). The highest and lowest per-patient specificity was observed for MRI (94%, 95% CI: 79-99) and for CCTA (39%, 95% CI: 34-44), respectively. Similar specificities were noted for SPECT (78%, 95% CI: 68-87), SE (75%, 95% CI: 63-85), FFRCT (71%, 95% CI: 65-75%), and ICA (67%, 95% CI: 63-71). On a per-vessel basis, the highest sensitivity was for CCTA (pooled sensitivity, 91%: 88-93), MRI (91%: 84-95), and FFRCT (83%, 78-87), with lower sensitivities for ICA (71%, 69-74), and SPECT (57%: 49-64). Per-vessel specificity was highest for MRI (85%, 79-89), FFRCT (78%: 78-81), and SPECT (75%: 69-80), whereas ICA (66%: 64-68) and CCTA (58%: 55-61) yielded a lower specificity.
Conclusions: In this meta-analysis comparing cardiac imaging methods directly to FFR, MRI had the highest performance for diagnosis of ischaemia-causing CAD, with lower performance for SPECT and SE. Anatomic methods of CCTA and ICA yielded lower specificity, with functional assessment of coronary atherosclerosis by SE, SPECT, and FFRCT improving accuracy.
Keywords: Cardiac imaging; Diagnostic accuracy; Fractional flow reserve; Meta-analysis.
© The Author 2016. Published by Oxford University Press on behalf of the European Society of Cardiology
Figures
Comment in
-
The impacts on healthcare when coronary angiography as the reference method for diagnostic accuracy of coronary artery disease is replaced by fractional flow reserve!Eur Heart J. 2017 Apr 1;38(13):999-1001. doi: 10.1093/eurheartj/ehw123. Eur Heart J. 2017. PMID: 27143782 No abstract available.
References
-
- Pijls NH, De Bruyne B, Peels K, Van Der Voort PH, Bonnier HJ, Bartunek J, Koolen JJ, Koolen JJ. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N Engl J Med 1996;334:1703–1708. - PubMed
-
- Authors/Task Force Members Windecker S, Kolh P, Alfonso F, Collet JP, Cremer J, Falk V, Filippatos G, Hamm C, Head SJ, Juni P, Kappetein AP, Kastrati A, Knuuti J, Landmesser U, Laufer G, Neumann FJ, Richter DJ, Schauerte P, Sousa Uva M, Stefanini GG, Taggart DP, Torracca L, Valgimigli M, Wijns W, Witkowski A. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J 2014;35:2541–2619. - PubMed
-
- Fihn SD, Blankenship JC, Alexander KP, Bittl JA, Byrne JG, Fletcher BJ, Fonarow GC, Lange RA, Levine GN, Maddox TM, Naidu SS, Ohman EM, Smith PK. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2014;64:1929–1949. - PubMed
-
- Tonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F, van’ t Veer M, Klauss V, Manoharan G, Engstrom T, Oldroyd KG, Ver Lee PN, MacCarthy PA, Fearon WF, Investigators FS. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med 2009;360:213–224. - PubMed
-
- Pijls NH, Fearon WF, Tonino PA, Siebert U, Ikeno F, Bornschein B, van't Veer M, Klauss V, Manoharan G, Engstrom T, Oldroyd KG, Ver Lee PN, MacCarthy PA, De Bruyne B, Investigators FS. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention in patients with multivessel coronary artery disease: 2-year follow-up of the FAME (Fractional Flow Reserve Versus Angiography for Multivessel Evaluation) study. J Am Coll Cardiol 2010;56:177–184. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
